Originally published Dec. 25, 2004, in the Tracy Press.
Touted as the “gold standard” procedure, Roux en Y — often called RNY for short — is considered by my insurer as the only surgical weight-loss method that has proven success. Two celebrities — former talk show host and singer Carnie Wilson and NBC weatherman Al Roker — both used this procedure to lose weight.This procedure will drastically alter the size and capacity of my stomach and reroute my digestive tract.
Weight-loss surgery is a big decision.When I was talking myself into the idea of sharing my story with readers, I told myself that if it prevented one person with unrealistic expectations from having the surgery, it would be a good thing. Now, I realize that I also want to help people who may truly need the surgery but are unaware of how to obtain it.For me, deciding whether to have surgery was difficult, but picking the procedure from the handful available was easy — my insurer only covered one.
Touted as the “gold standard” procedure, Roux en Y — often called RNY for short — is considered by my insurer as the only surgical weight-loss method that has proven success. Two celebrities — former talk show host and singer Carnie Wilson and NBC weatherman Al Roker — both used this procedure to lose weight.This procedure will drastically alter the size and capacity of my stomach and reroute my digestive tract.
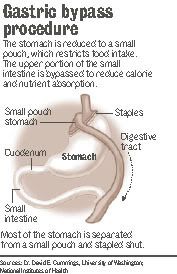
My new stomach will be a thumb-sized pouch that connects to about 18 inches of lower intestine. The pouch will stretch to the size of a chicken egg to accommodate food. The procedure is called gastric bypass because much of the gastric system is bypassed.The digestive tract becomes like a sink. Food goes down the drain of the esophagus into the stomach and then empties through another drain into the intestines before it exits the body. The drains are about the size of a dime.
Aside from preventing me from eating much in one sitting and significantly limiting my feelings of hunger, this procedure also will cause unpleasant side effects if I don’t follow the rules. If I don’t chew my food well enough, it will either block the opening between my esophagus and pouch or plug the outlet from my pouch to intestine. Usually, there are two solutions to this problem: vomiting or having a doctor use an endoscope to remove the blockage. Neither sounds like fun to me.
If I eat foods with too much sugar or fat, I may experience dumping syndrome. A phenomenon experienced by about 15 percent of all RNY patients, dumping is described by doctors and former patients as “behavior modification with a vengeance.” The syndrome occurs when a high concentration of sugar or fat is dumped into the intestine. It manifests itself in different ways, but often causes reactions similar to hypoglycemia, such as sweating, feeling faint, heart palpitations and an overwhelming need to lie down. The idea is that after patients experience dumping syndrome once or twice, they stay away from foods loaded with sugar or fat permanently.After surgery, my main dietary focus will be protein.
For the first few weeks with my new digestive system, I will only be able to eat one to two ounces three times a day. That’s not a lot of food. So I will have to work very hard to get in as much protein as possible.
If I don’t get enough protein, I will suffer brittle nails, scaly skin and baldness. I don’t plan to go through this ordeal to end up looking like the Crypt Keeper. Protein also helps maintain muscle mass and the feeling of being satisfied after a meal. I’ll supplement my limited food consumption with a host of vitamins. I’ll take a high-potency multivitamin, calcium and iron every day for the rest of my life. I will also take vitamin B12 under my tongue twice a week because my body will no longer be able to absorb the vitamin through my digestive tract.Vitamin deficiency is linked to permanent hair loss, anemia, hearing loss and other neurological disorders. I’ve already warned my husband that if I start looking AND acting like the Crypt Keeper, crushing up some chewable vitamins in a protein shake should do the trick.
In all seriousness, a lot of work is involved on the part of the patient to ensure the success of gastric bypass.This is not a passive cure-all.As you can see, I will suffer some serious consequences if I don’t follow the post-operative program to the letter.The end-all nature of this is a scary thought for me. I’m the one who has gained and lost the equivalent of two average-sized people in my short time on this planet.What makes me think this time is different? The short answer is: because it has to be. The long answer is fodder for another column, maybe one I’ll write next week.
