Originally published Jan. 29, 2005, in the Tracy Press
A little over a month ago, I began writing this column with the idea that I would have gastric- bypass surgery sometime between March and August of this year.
It’s amazing to me how so much can change in what feels like the blink of an eye. It turns out that in just four short weeks from now, I will go under the knife to have my digestive system rerouted to facilitate rapid weight loss — to the tune of about 100 pounds in the first year — in the hopes of overcoming obesity-related infertility.
It’s almost surreal as I think back to how this occurred.
A few weeks ago, I was crying in my soup about how the holidays were a little too festive for me. I talked about how I needed to get back on track because I was meeting with the hospital bariatric team’s medical director, and I wanted to make a good impression by not gaining weight. I succeeded in that. Turns out my scale at home was closer to the hospital scale than I realized, and I weighed in four pounds lighter than in early December. Not too shabby for having a one-week detour around Christmas.
The medical director and I hit it off instantly. We discussed my weight history and the eating habits I learned as a child. She explained her take on my experiences. We talked a bit about my medical history.
And then she said it: “So, Tonya, when would you like to have surgery?”
Stunned, I said, “March?,” thinking she wanted to give me some sort of timeline.
Instead, she said, “You got it.”
I almost couldn’t speak. I managed to stutter, “really?”
Her answer knocked my socks off.
“Well, you’ve lost weight, you’re making life changes, and you don’t have any medical conditions barring you from surgery. You’re a good candidate. Why should we postpone it?”
It’s one thing to believe you’ve earned something, but it’s an entirely different feeling to have the person in control of your reward validate it.
It turns out that March didn’t exactly work out, and I now have a Feb. 24 surgery date. I wasn’t sure whether to jump for joy or burst into tears.
My poor husband wasn’t sure how to take it either. I was so frazzled by the news that I couldn’t even fill out my pre-op forms. He had to do it for me.
Walking out of the office, into the elevator, down four floors and out of the building seemed like a dream.
I don’t think the magnitude of what just happened hit me until the drive home. And then it just exhausted me. I couldn’t stop thinking of everything that needed to be done before surgery.
Some things were little, but everything seemed like a huge boulder of effort.
As soon as we got home, I went straight to the bedroom to lie down. I slept for four hours. The only time I can ever remember sleeping like that was in college the night before I had five difficult finals in the same day. It’s that heavy, drugged sleep your body goes into when your brain is so full of information that you have to be nearly comatose for it to be assimilated.
When I awoke, I was groggy, and everything was still jumbled in my brain. I decided to make myself a late dinner and watch a dumb movie with my husband. I can’t even remember what we watched.
Then, we went to bed. He fell asleep, and I took out my information binder that I was given at my pre-operative orientation in October. I read the entire three-inch binder word for word. Then
I went back to sleep. The next day, I freaked out a little more, repeatedly rattling off everything that had to be done before surgery — balance the checkbook, request time off from work, inform my staff of my upcoming month-long absence and about 50 billion other things I can’t mention here. I must have sounded like Dustin Hoffman in “Rainman,” as I muttered under my breath.
Finally, I took a friend’s advice and made myself a list of everything that needed to be done. Many people have offered to help me, but I’ve yet to take anyone up on it.
After this week, I’ll have three more columns to publish before the day of surgery, and I’ll have to prewrite at least two for part of the time I’m recovering. That gives me five chances to tell readers about my preparations. It doesn’t feel like nearly enough but I’ll give it my best shot.
Saturday, January 29, 2005
Saturday, January 22, 2005
What I miss
Originally published Jan. 22, 2005, in the Tracy Press
Last week’s column discussed everything I’m no longer allowed to eat as I prepare to have gastric-bypass surgery. I’ve begun living as if I’ve already had the surgery, which includes abstaining from a host of no-no foods.
When I was considering surgery about a year ago, I realized that I needed to make sure I could live without all my favorites. If I couldn’t live without food that would be verboten, then there was no point in having weight-loss surgery.
I made myself a list of the foods I didn’t think I’d be able to live without forever, and I proceeded to test them. I would prepare the item or order it in a restaurant and reflect on it. I’d take a bite and see if it really tasted as good as I thought it did. I’d see if it felt good on my tongue and whether it felt generally good to eat it.
Surprisingly, most things haven’t been that hard to give up. But I think others will be a challenge for the rest of my life. I’m willing to take the challenge because I believe the benefits of surgery are worth it.
Here’s a rundown of what I found:
What I don’t miss
• Soda — I hadn’t really liked soda as a child, so giving it up was easy.
• Carbonation — As much as I love mineral water, I don’t miss it.
• Gum — I still think Dentyne Ice is the best remedy for after-lunch breath, but sugar-free breath mints will suffice.
• Coconut — The only time I eat coconut is when it’s in candy or desserts, and those are already forbidden (more on that later).
• Beef jerky — Since I don’t eat beef, it’s a non-issue.
What I do miss
• Alcohol — Drinking water at a party seems to make more of a spectacle of me than the drunken girl who dances topless on the bar.
• Fast food — I don’t actually miss the flavor of fast food (except for the grilled-cheese sandwich at In-N-Out), but I do miss the convenience of hitting a drive-through window when I’m short on time.
• Bread — The only reason I miss bread is because it’s very hard to make a sandwich without any.
• Pasta — As if I can imagine going to The Olive Garden and ordering anything else. I really don’t like minestrone soup, so this may be a restaurant I don’t eat at after surgery.
• Rice — Tofu curry from the Thai Café on Central Avenue just doesn’t taste good when it’s not combined with jasmine rice.
• Spicy food — Mild salsa just doesn’t enhance Mexican food as well as the hotter varieties.
• Desserts — This is almost deserving of its own column. I love desserts. Anything sweet and creamy has my vote. Cover it in chocolate and I consider it unbeatable.
I have to be honest: That list I made about a year ago specifying all the foods I wanted to see if I could live without consisted almost entirely of desserts. Sure, the In-N-Out grilled cheese was on the list, but it only took one bite for me to realize that I could live the rest of my life without eating another one. The chocolate mousse cake from Fabio’s, on the other hand, took three tries before I could resign myself to the idea of living without it (Yes, it really is that good).
I couldn’t begin to discuss my love for rich desserts, particularly when paired with a glass of vintage port wine. No dessert has ever been too rich for me — not even the decadent chocolate truffle pie at Magellan’s.
Even fast food — which I subsisted on for at least five days a week — wasn’t as hard to give up.
The deciding factor for me going through with gastric-bypass surgery is the realization that food is fleeting.
Yes, I love Marie Callender’s pies and the blended Carmelo Sensation at Zizzo’s on 10th Street. But I love the idea of fitting into the seats on amusement park rides so much more. The idea of climbing up the rock formations at Mount Diablo with my husband is as intoxicating as any ice cream creation at Cold Stone Creamery.
And the best feeling I can imagine is becoming pregnant and giving birth to my own child. And I know that won’t happen for me without surgery.
When it comes to the idea of having a baby, the richest dessert in the world holds no comparison.
Last week’s column discussed everything I’m no longer allowed to eat as I prepare to have gastric-bypass surgery. I’ve begun living as if I’ve already had the surgery, which includes abstaining from a host of no-no foods.
When I was considering surgery about a year ago, I realized that I needed to make sure I could live without all my favorites. If I couldn’t live without food that would be verboten, then there was no point in having weight-loss surgery.
I made myself a list of the foods I didn’t think I’d be able to live without forever, and I proceeded to test them. I would prepare the item or order it in a restaurant and reflect on it. I’d take a bite and see if it really tasted as good as I thought it did. I’d see if it felt good on my tongue and whether it felt generally good to eat it.
Surprisingly, most things haven’t been that hard to give up. But I think others will be a challenge for the rest of my life. I’m willing to take the challenge because I believe the benefits of surgery are worth it.
Here’s a rundown of what I found:
What I don’t miss
• Soda — I hadn’t really liked soda as a child, so giving it up was easy.
• Carbonation — As much as I love mineral water, I don’t miss it.
• Gum — I still think Dentyne Ice is the best remedy for after-lunch breath, but sugar-free breath mints will suffice.
• Coconut — The only time I eat coconut is when it’s in candy or desserts, and those are already forbidden (more on that later).
• Beef jerky — Since I don’t eat beef, it’s a non-issue.
What I do miss
• Alcohol — Drinking water at a party seems to make more of a spectacle of me than the drunken girl who dances topless on the bar.
• Fast food — I don’t actually miss the flavor of fast food (except for the grilled-cheese sandwich at In-N-Out), but I do miss the convenience of hitting a drive-through window when I’m short on time.
• Bread — The only reason I miss bread is because it’s very hard to make a sandwich without any.
• Pasta — As if I can imagine going to The Olive Garden and ordering anything else. I really don’t like minestrone soup, so this may be a restaurant I don’t eat at after surgery.
• Rice — Tofu curry from the Thai Café on Central Avenue just doesn’t taste good when it’s not combined with jasmine rice.
• Spicy food — Mild salsa just doesn’t enhance Mexican food as well as the hotter varieties.
• Desserts — This is almost deserving of its own column. I love desserts. Anything sweet and creamy has my vote. Cover it in chocolate and I consider it unbeatable.
I have to be honest: That list I made about a year ago specifying all the foods I wanted to see if I could live without consisted almost entirely of desserts. Sure, the In-N-Out grilled cheese was on the list, but it only took one bite for me to realize that I could live the rest of my life without eating another one. The chocolate mousse cake from Fabio’s, on the other hand, took three tries before I could resign myself to the idea of living without it (Yes, it really is that good).
I couldn’t begin to discuss my love for rich desserts, particularly when paired with a glass of vintage port wine. No dessert has ever been too rich for me — not even the decadent chocolate truffle pie at Magellan’s.
Even fast food — which I subsisted on for at least five days a week — wasn’t as hard to give up.
The deciding factor for me going through with gastric-bypass surgery is the realization that food is fleeting.
Yes, I love Marie Callender’s pies and the blended Carmelo Sensation at Zizzo’s on 10th Street. But I love the idea of fitting into the seats on amusement park rides so much more. The idea of climbing up the rock formations at Mount Diablo with my husband is as intoxicating as any ice cream creation at Cold Stone Creamery.
And the best feeling I can imagine is becoming pregnant and giving birth to my own child. And I know that won’t happen for me without surgery.
When it comes to the idea of having a baby, the richest dessert in the world holds no comparison.
Saturday, January 15, 2005
What not to eat
Originally published Jan. 15, 2005.
I mentioned last week that I have to start living my life as if I have already had gastric-bypass surgery. This means, I must exercise regularly and eat differently.
Exercising regularly is a no-brainer. I’m expected to exercise at least 30 minutes a day, six days a week. This will help get my body in shape to recover faster from surgery. Exercising regularly now also means that I’ll be more able to increase my workouts after surgery. Most patients I’ve spoken to exercise one to two hours a day, six days a week.
Having spent much of my life trying to control my weight, I’m familiar with exercise.
I like doing yoga and lifting weights. Pilates is fun, but I have trouble completing an hour-long session. Cardio is my least favorite form of exercise, but I have grown to enjoy using an elliptical cross-trainer at the gym. The zero-impact motion is easy on my knees without being too easy on the rest of me.
I’ve been told cardiovascular exercise will help my body better handle the effects of anesthesia, though I have yet to confirm this with a surgeon; however, doctors have told me that strength training now will help me to preserve my muscle mass during recovery. Building my stomach muscles should also help my abdominal wall heal from the incision wounds faster.
Aside from needing to be better about scheduling my workout as if it were any other unbreakable appointment, I’ve gotten the exercise component down pat.
The more difficult aspect of preparing for surgery is eating differently. I’ve grown accustomed to my new eating habits and am comfortable with them now, but that wasn’t the case three months ago when I received my pre-operative eating requirements.
Except for the week of Christmas, I’ve diligently followed my prescribed 1,200- calorie-a-day eating plan for the past 12 weeks. As I touched on last week, though, there is a lot more to my new plan than just watching calories.
Limiting myself to 1,200 calories a day and making sure I consume 80 grams of protein, 133 grams of carbohydrate and no more than 40 grams of fat is easy. But there’s a whole list of rules accompanying that seemingly easy meal plan that is more difficult.
The rules are there to prepare me for life “on the other side.” As such, they don’t make a lot of sense for my body now, but I’m getting ready for when they really do matter.
Here’s a rundown:
• No snacking — I’m supposed to fully fill my pouch at mealtime three times a day. Doing so will enable me to go about five hours between meals with little feeling of hunger.
• No fast foods — Healthy food can be found at fast-food restaurants. But the sights and smells of McDonald’s and Jack In the Box are triggers. For many of us, it’s hard to walk in or go to the drive-through window and only order a salad.
• No caffeine — The stomach pouch has little to no stomach acid. With no acid to dilute it, caffeine could very quickly ulcerate the pouch.
• No carbonated beverages — Carbonation will add gas to the stomach pouch, which can stretch it and enable it to hold more food. Not so good if the idea is to restrict the amount of food consumed in one sitting. Stretching the pouch is also bad because if it’s done too soon after surgery, the staple line could rupture.
• No fluids with meals — This is another rule to help keep the pouch full as long as possible to maintain the feeling of satisfaction. If fluids are consumed with meals, the pouch may empty faster, which means I could eat more in one sitting.
• Avoid starches — Bread gets doughy in the pouch and can clog the outlet, which would be very uncomfortable and could require medical attention to clear.
Because the opening from the pouch to the intestine is only the size of a dime, food must be chewed to the consistency of baby food. Some foods, however, are too difficult to chew that well. These foods include coconut, popcorn, corn and skins and seeds of fruit.
When I first encountered all these rules, I remember thinking that there was no way I could go through with the surgery. There were too many foods I’d have to avoid that I swore I could never live without. But I’ve managed for the last three months, and I don’t miss many of the things I thought I would.
How did I accomplish this? That’s what next week’s column is about.
I mentioned last week that I have to start living my life as if I have already had gastric-bypass surgery. This means, I must exercise regularly and eat differently.
Exercising regularly is a no-brainer. I’m expected to exercise at least 30 minutes a day, six days a week. This will help get my body in shape to recover faster from surgery. Exercising regularly now also means that I’ll be more able to increase my workouts after surgery. Most patients I’ve spoken to exercise one to two hours a day, six days a week.
Having spent much of my life trying to control my weight, I’m familiar with exercise.
I like doing yoga and lifting weights. Pilates is fun, but I have trouble completing an hour-long session. Cardio is my least favorite form of exercise, but I have grown to enjoy using an elliptical cross-trainer at the gym. The zero-impact motion is easy on my knees without being too easy on the rest of me.
I’ve been told cardiovascular exercise will help my body better handle the effects of anesthesia, though I have yet to confirm this with a surgeon; however, doctors have told me that strength training now will help me to preserve my muscle mass during recovery. Building my stomach muscles should also help my abdominal wall heal from the incision wounds faster.
Aside from needing to be better about scheduling my workout as if it were any other unbreakable appointment, I’ve gotten the exercise component down pat.
The more difficult aspect of preparing for surgery is eating differently. I’ve grown accustomed to my new eating habits and am comfortable with them now, but that wasn’t the case three months ago when I received my pre-operative eating requirements.
Except for the week of Christmas, I’ve diligently followed my prescribed 1,200- calorie-a-day eating plan for the past 12 weeks. As I touched on last week, though, there is a lot more to my new plan than just watching calories.
Limiting myself to 1,200 calories a day and making sure I consume 80 grams of protein, 133 grams of carbohydrate and no more than 40 grams of fat is easy. But there’s a whole list of rules accompanying that seemingly easy meal plan that is more difficult.
The rules are there to prepare me for life “on the other side.” As such, they don’t make a lot of sense for my body now, but I’m getting ready for when they really do matter.
Here’s a rundown:
• No snacking — I’m supposed to fully fill my pouch at mealtime three times a day. Doing so will enable me to go about five hours between meals with little feeling of hunger.
• No fast foods — Healthy food can be found at fast-food restaurants. But the sights and smells of McDonald’s and Jack In the Box are triggers. For many of us, it’s hard to walk in or go to the drive-through window and only order a salad.
• No caffeine — The stomach pouch has little to no stomach acid. With no acid to dilute it, caffeine could very quickly ulcerate the pouch.
• No carbonated beverages — Carbonation will add gas to the stomach pouch, which can stretch it and enable it to hold more food. Not so good if the idea is to restrict the amount of food consumed in one sitting. Stretching the pouch is also bad because if it’s done too soon after surgery, the staple line could rupture.
• No fluids with meals — This is another rule to help keep the pouch full as long as possible to maintain the feeling of satisfaction. If fluids are consumed with meals, the pouch may empty faster, which means I could eat more in one sitting.
• Avoid starches — Bread gets doughy in the pouch and can clog the outlet, which would be very uncomfortable and could require medical attention to clear.
Because the opening from the pouch to the intestine is only the size of a dime, food must be chewed to the consistency of baby food. Some foods, however, are too difficult to chew that well. These foods include coconut, popcorn, corn and skins and seeds of fruit.
When I first encountered all these rules, I remember thinking that there was no way I could go through with the surgery. There were too many foods I’d have to avoid that I swore I could never live without. But I’ve managed for the last three months, and I don’t miss many of the things I thought I would.
How did I accomplish this? That’s what next week’s column is about.
Saturday, January 08, 2005
Getting back on track
Originally published Jan. 8, 2005, in the Tracy Press.
As the first week of the new year comes to a close, I have to say I spent it like most people — making up for the sins of the holidays.
What many refer to as a New Year’s resolution is a means to an end for me. I need to lose about 30 pounds to be cleared for gastric-bypass surgery through my insurer. I was given that weight goal at my pre-operative orientation in mid- October. Between that day and my visit with the program’s dietician in early December, I had lost nine pounds. The dietician seemed impressed, especially considering that I met with her the week after Thanksgiving.
Unfortunately, the week of Christmas brought a setback. It’s never the day of the holiday that gets me. With plenty of people to visit with, I find myself too distracted to overeat. What seems to be my downfall is the time preceding a holiday, when I’m too scatterbrained to pay attention to what I’m putting in my mouth. And I tend to lose my resolve at work.
Holidays are a tough time in most offices — everyone is doing extra work to make up for the shorter workweeks or to fill in for those on vacation, not to mention dealing with the seemingly endless supply of treats dropped off by clients or brought in by co-workers.
After giving in to a truffle, it became easier to say yes to fudge, cookies and gourmet coffee drinks. And the easier it was to say yes, the harder it was to say no. And that’s why I spent Christmas night realizing that the jeans that had been so loose the week before now protested every time I tried to lift the zipper.
I spent much of last week thinking about how I was going to get back on track. It felt like I had all the time in the world — until I pulled out my 2005 calendar and realized I had a little more than a week before my next weigh-in.
As you read this column, I will be on my way to San Francisco to meet with the bariatric program director at the hospital where I’m expected to have surgery.
The director has the power to schedule my surgery for two weeks — or even two years — from when we meet. Showing up with a 10-pound gain is not the way to convey that I’m serious about having surgery.
I’ve had to kick my butt into high gear. I know fad diets don’t work, so I haven’t spent the week fasting or eating nothing but cabbage soup.
I’ve gone back to the preoperative eating plan prescribed by the bariatric team in charge of my case.
Yes, not only do I have to lose weight before surgery, but I’m expected to do it a certain way. The hospital’s way consists of eating 1,200 calories a day in the form of three balanced meals.
Calories aren’t the only thing I have to watch. The bariatric doctors want me to begin living life as if I already have had the surgery. Doing so is meant to prevent me from having transition difficulties after surgery, because not following the dietary rules could kill me.
Within my 1,200 calories a day, I need to consume between 75 and 90 grams of protein, up to 40 grams of fat and no more than 133 grams of carbohydrates.
Though this plan is low in carbs, it’s not a low-carb diet in the traditional sense, because fat and calories are also limited. It’s a low-calorie, low-carb, high-protein and moderate-fat plan.
For the first year after surgery, I will eat anywhere from 500 to 900 calories a day.
Cutting my consumption down to 1,200 now will be a good way to get my body used to reduced nutrients.
The anatomical limitations I’ll have after surgery will prevent me from digesting starchy foods very well, and cutting carbs is better done now than later.
As I’ve explained before, protein will be my main concern after surgery, and it’s best that I focus my energy on lean sources now so I’ll have an easier time later. Not eating red meat or poultry makes it more of challenge, but I’m working on it.
I’m also expected to replace one meal a day with a sugar-free protein supplement that I’m allowed to mix with either milk or water.
Other rules meant to prepare me for surgery include no carbonated beverages, no caffeine and no alcohol.
I’ll tell you a little more about what I can and can’t eat next week. But for now, I need to head to the gym — more on that later, too.
As the first week of the new year comes to a close, I have to say I spent it like most people — making up for the sins of the holidays.
What many refer to as a New Year’s resolution is a means to an end for me. I need to lose about 30 pounds to be cleared for gastric-bypass surgery through my insurer. I was given that weight goal at my pre-operative orientation in mid- October. Between that day and my visit with the program’s dietician in early December, I had lost nine pounds. The dietician seemed impressed, especially considering that I met with her the week after Thanksgiving.
Unfortunately, the week of Christmas brought a setback. It’s never the day of the holiday that gets me. With plenty of people to visit with, I find myself too distracted to overeat. What seems to be my downfall is the time preceding a holiday, when I’m too scatterbrained to pay attention to what I’m putting in my mouth. And I tend to lose my resolve at work.
Holidays are a tough time in most offices — everyone is doing extra work to make up for the shorter workweeks or to fill in for those on vacation, not to mention dealing with the seemingly endless supply of treats dropped off by clients or brought in by co-workers.
After giving in to a truffle, it became easier to say yes to fudge, cookies and gourmet coffee drinks. And the easier it was to say yes, the harder it was to say no. And that’s why I spent Christmas night realizing that the jeans that had been so loose the week before now protested every time I tried to lift the zipper.
I spent much of last week thinking about how I was going to get back on track. It felt like I had all the time in the world — until I pulled out my 2005 calendar and realized I had a little more than a week before my next weigh-in.
As you read this column, I will be on my way to San Francisco to meet with the bariatric program director at the hospital where I’m expected to have surgery.
The director has the power to schedule my surgery for two weeks — or even two years — from when we meet. Showing up with a 10-pound gain is not the way to convey that I’m serious about having surgery.
I’ve had to kick my butt into high gear. I know fad diets don’t work, so I haven’t spent the week fasting or eating nothing but cabbage soup.
I’ve gone back to the preoperative eating plan prescribed by the bariatric team in charge of my case.
Yes, not only do I have to lose weight before surgery, but I’m expected to do it a certain way. The hospital’s way consists of eating 1,200 calories a day in the form of three balanced meals.
Calories aren’t the only thing I have to watch. The bariatric doctors want me to begin living life as if I already have had the surgery. Doing so is meant to prevent me from having transition difficulties after surgery, because not following the dietary rules could kill me.
Within my 1,200 calories a day, I need to consume between 75 and 90 grams of protein, up to 40 grams of fat and no more than 133 grams of carbohydrates.
Though this plan is low in carbs, it’s not a low-carb diet in the traditional sense, because fat and calories are also limited. It’s a low-calorie, low-carb, high-protein and moderate-fat plan.
For the first year after surgery, I will eat anywhere from 500 to 900 calories a day.
Cutting my consumption down to 1,200 now will be a good way to get my body used to reduced nutrients.
The anatomical limitations I’ll have after surgery will prevent me from digesting starchy foods very well, and cutting carbs is better done now than later.
As I’ve explained before, protein will be my main concern after surgery, and it’s best that I focus my energy on lean sources now so I’ll have an easier time later. Not eating red meat or poultry makes it more of challenge, but I’m working on it.
I’m also expected to replace one meal a day with a sugar-free protein supplement that I’m allowed to mix with either milk or water.
Other rules meant to prepare me for surgery include no carbonated beverages, no caffeine and no alcohol.
I’ll tell you a little more about what I can and can’t eat next week. But for now, I need to head to the gym — more on that later, too.
Saturday, January 01, 2005
What makes this time different?
Originally published Jan. 1, 2005, in the Tracy Press.
I ask myself that question all the time. As I mentioned last week, the immediate answer I come up with is: because it has to be.
But that doesn’t really answer the question of what it is about surgical weight loss that makes me think it’ll work when every other diet on the planet has failed.
I hate to sound cliché, but there’s a lot to be said for the journey making all the difference in the world.
I consider myself in a fortunate place right now. I found myself abruptly switching insurance providers last summer just as I was exploring the possibilities of surgical weight loss.
My new insurer is a health maintenance organization with a five-year-old program devoted to weight-loss surgery.
Though weight-loss surgery has been around since the 1970s, few insurers actually have programs in place for members seeking it. It seems more common that insurers require nothing more than a doctor’s referral and leave surgery preparation up to the bariatric specialists with whom they contract.
Every member of my HMO seeking WLS must submit to a process that takes anywhere from 12 to 18 months. The process includes nutrition classes, psychological counseling and lab work — and that’s just to get a patient’s foot in the door.
Once that happens — meaning the HMO’s bariatric program agrees to accept the patient as a surgery candidate — there is still more work to be done.
Everyone must attend a bariatric orientation class at the hospital where he or she will have surgery. The orientation includes a weigh-in and a series of presentations by the hospital’s bariatric team. Patients are told the specifics of gastric-bypass surgery, its pros and cons and the most common complications. A large portion of the day is spent with a nutritionist explaining the vast differences between what patients can eat before surgery vs. after surgery.
The staff also lays down the rules for the program. The most common is a requirement for pre-operative weight loss.
I know it sounds silly, but my insurer expects all bariatric patients to lose 10 percent of their pre-operative weight before they can be cleared for surgery. I’ve heard different justifications for this requirement. Some say that weight-loss shrinks the size of liver, which is very close to the operation site and could be nicked during surgery. Others say it’s necessary because weight loss will reduce belly fat, and the amount of belly fat a person has determines whether surgery can be done laproscopically.
My opinion is that the surgery is expensive, and the HMO doesn’t want to invest its money in patients who aren’t willing to work at being successful. Requiring pre-op weight loss is a way to weed out those who are less than committed. I also believe that the insurer hopes that after losing about 30 pounds — the average patient weighs between 280 and 300 pounds — the patient will change his or her mind about needing surgery.
Some patients remove themselves from the program after orientation either because they don’t feel they can meet all the requirements or because they no longer believe that surgery is the right choice for them. Those who don’t are required to attend further meetings with bariatric nutritionists, psychologists and specialists to make sure they have realistic expectations of surgery and that they are good candidates for surgery. Being a good candidate for surgery, according to my insurer, means the patient is likely to survive the procedure.
As one surgeon told me, “If we’re going to operate, we’d like to be at least 90 percent certain that you’ll wake up when we’re done.”
Apparently, having patients die doesn’t make surgeons very happy.
It’s only after losing 10 percent of their weight and submitting to about a dozen different appointments that patients are truly cleared for surgery and a date is scheduled.
I’m in the midst of this process, and though it can be daunting, I find it comforting.
As someone who has spent thousands of dollars on diet programs, books and pills, I like the fact that I have to work at this. And every obstacle I pass in this process validates that I’m making the right decision.
I attended orientation in October and am now focused on losing about 30 pounds. I did really well in November, dropping nine pounds.
However, the stress of Christmas got the better of me, and I put a bit of that back on.
When I visited the bariatric nutritionist in early December, she told me I was an excellent candidate for fast-tracking, which means I could have the surgery sooner rather than later. She predicted I may have surgery as early as March.
However, I have an appointment Jan. 8 with the program’s medical director. She’s the one who determines whether I get put on that fast track. If I don’t have at least 10 pounds lost by the time I see her, my chances of being fast-tracked are slim.
My focus now is getting back on track. That’s not easy after two weeks of absent-minded indulgence, but it’s a challenge I’m ready to take on.
I ask myself that question all the time. As I mentioned last week, the immediate answer I come up with is: because it has to be.
But that doesn’t really answer the question of what it is about surgical weight loss that makes me think it’ll work when every other diet on the planet has failed.
I hate to sound cliché, but there’s a lot to be said for the journey making all the difference in the world.
I consider myself in a fortunate place right now. I found myself abruptly switching insurance providers last summer just as I was exploring the possibilities of surgical weight loss.
My new insurer is a health maintenance organization with a five-year-old program devoted to weight-loss surgery.
Though weight-loss surgery has been around since the 1970s, few insurers actually have programs in place for members seeking it. It seems more common that insurers require nothing more than a doctor’s referral and leave surgery preparation up to the bariatric specialists with whom they contract.
Every member of my HMO seeking WLS must submit to a process that takes anywhere from 12 to 18 months. The process includes nutrition classes, psychological counseling and lab work — and that’s just to get a patient’s foot in the door.
Once that happens — meaning the HMO’s bariatric program agrees to accept the patient as a surgery candidate — there is still more work to be done.
Everyone must attend a bariatric orientation class at the hospital where he or she will have surgery. The orientation includes a weigh-in and a series of presentations by the hospital’s bariatric team. Patients are told the specifics of gastric-bypass surgery, its pros and cons and the most common complications. A large portion of the day is spent with a nutritionist explaining the vast differences between what patients can eat before surgery vs. after surgery.
The staff also lays down the rules for the program. The most common is a requirement for pre-operative weight loss.
I know it sounds silly, but my insurer expects all bariatric patients to lose 10 percent of their pre-operative weight before they can be cleared for surgery. I’ve heard different justifications for this requirement. Some say that weight-loss shrinks the size of liver, which is very close to the operation site and could be nicked during surgery. Others say it’s necessary because weight loss will reduce belly fat, and the amount of belly fat a person has determines whether surgery can be done laproscopically.
My opinion is that the surgery is expensive, and the HMO doesn’t want to invest its money in patients who aren’t willing to work at being successful. Requiring pre-op weight loss is a way to weed out those who are less than committed. I also believe that the insurer hopes that after losing about 30 pounds — the average patient weighs between 280 and 300 pounds — the patient will change his or her mind about needing surgery.
Some patients remove themselves from the program after orientation either because they don’t feel they can meet all the requirements or because they no longer believe that surgery is the right choice for them. Those who don’t are required to attend further meetings with bariatric nutritionists, psychologists and specialists to make sure they have realistic expectations of surgery and that they are good candidates for surgery. Being a good candidate for surgery, according to my insurer, means the patient is likely to survive the procedure.
As one surgeon told me, “If we’re going to operate, we’d like to be at least 90 percent certain that you’ll wake up when we’re done.”
Apparently, having patients die doesn’t make surgeons very happy.
It’s only after losing 10 percent of their weight and submitting to about a dozen different appointments that patients are truly cleared for surgery and a date is scheduled.
I’m in the midst of this process, and though it can be daunting, I find it comforting.
As someone who has spent thousands of dollars on diet programs, books and pills, I like the fact that I have to work at this. And every obstacle I pass in this process validates that I’m making the right decision.
I attended orientation in October and am now focused on losing about 30 pounds. I did really well in November, dropping nine pounds.
However, the stress of Christmas got the better of me, and I put a bit of that back on.
When I visited the bariatric nutritionist in early December, she told me I was an excellent candidate for fast-tracking, which means I could have the surgery sooner rather than later. She predicted I may have surgery as early as March.
However, I have an appointment Jan. 8 with the program’s medical director. She’s the one who determines whether I get put on that fast track. If I don’t have at least 10 pounds lost by the time I see her, my chances of being fast-tracked are slim.
My focus now is getting back on track. That’s not easy after two weeks of absent-minded indulgence, but it’s a challenge I’m ready to take on.
Saturday, December 25, 2004
The procedure explained
Originally published Dec. 25, 2004, in the Tracy Press.
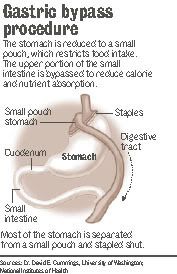
Touted as the “gold standard” procedure, Roux en Y — often called RNY for short — is considered by my insurer as the only surgical weight-loss method that has proven success. Two celebrities — former talk show host and singer Carnie Wilson and NBC weatherman Al Roker — both used this procedure to lose weight.This procedure will drastically alter the size and capacity of my stomach and reroute my digestive tract.
Weight-loss surgery is a big decision.When I was talking myself into the idea of sharing my story with readers, I told myself that if it prevented one person with unrealistic expectations from having the surgery, it would be a good thing. Now, I realize that I also want to help people who may truly need the surgery but are unaware of how to obtain it.For me, deciding whether to have surgery was difficult, but picking the procedure from the handful available was easy — my insurer only covered one.
Touted as the “gold standard” procedure, Roux en Y — often called RNY for short — is considered by my insurer as the only surgical weight-loss method that has proven success. Two celebrities — former talk show host and singer Carnie Wilson and NBC weatherman Al Roker — both used this procedure to lose weight.This procedure will drastically alter the size and capacity of my stomach and reroute my digestive tract.
My new stomach will be a thumb-sized pouch that connects to about 18 inches of lower intestine. The pouch will stretch to the size of a chicken egg to accommodate food. The procedure is called gastric bypass because much of the gastric system is bypassed.The digestive tract becomes like a sink. Food goes down the drain of the esophagus into the stomach and then empties through another drain into the intestines before it exits the body. The drains are about the size of a dime.
Aside from preventing me from eating much in one sitting and significantly limiting my feelings of hunger, this procedure also will cause unpleasant side effects if I don’t follow the rules. If I don’t chew my food well enough, it will either block the opening between my esophagus and pouch or plug the outlet from my pouch to intestine. Usually, there are two solutions to this problem: vomiting or having a doctor use an endoscope to remove the blockage. Neither sounds like fun to me.
If I eat foods with too much sugar or fat, I may experience dumping syndrome. A phenomenon experienced by about 15 percent of all RNY patients, dumping is described by doctors and former patients as “behavior modification with a vengeance.” The syndrome occurs when a high concentration of sugar or fat is dumped into the intestine. It manifests itself in different ways, but often causes reactions similar to hypoglycemia, such as sweating, feeling faint, heart palpitations and an overwhelming need to lie down. The idea is that after patients experience dumping syndrome once or twice, they stay away from foods loaded with sugar or fat permanently.After surgery, my main dietary focus will be protein.
For the first few weeks with my new digestive system, I will only be able to eat one to two ounces three times a day. That’s not a lot of food. So I will have to work very hard to get in as much protein as possible.
If I don’t get enough protein, I will suffer brittle nails, scaly skin and baldness. I don’t plan to go through this ordeal to end up looking like the Crypt Keeper. Protein also helps maintain muscle mass and the feeling of being satisfied after a meal. I’ll supplement my limited food consumption with a host of vitamins. I’ll take a high-potency multivitamin, calcium and iron every day for the rest of my life. I will also take vitamin B12 under my tongue twice a week because my body will no longer be able to absorb the vitamin through my digestive tract.Vitamin deficiency is linked to permanent hair loss, anemia, hearing loss and other neurological disorders. I’ve already warned my husband that if I start looking AND acting like the Crypt Keeper, crushing up some chewable vitamins in a protein shake should do the trick.
In all seriousness, a lot of work is involved on the part of the patient to ensure the success of gastric bypass.This is not a passive cure-all.As you can see, I will suffer some serious consequences if I don’t follow the post-operative program to the letter.The end-all nature of this is a scary thought for me. I’m the one who has gained and lost the equivalent of two average-sized people in my short time on this planet.What makes me think this time is different? The short answer is: because it has to be. The long answer is fodder for another column, maybe one I’ll write next week.
Saturday, December 18, 2004
A difficult decision made
Originally published Dec. 18, 2004, in the Tracy Press.
I’m officially under the gun to lose weight. I have obesity-related infertility, and if my husband and I hope to conceive the old fashioned way, I need to drop at least 100 pounds. And my doctor suggests I do it sooner rather than later. That’s no easy undertaking.After all, only 5 percent of Americans who diet are successful at maintaining weight loss. I’ve never been among that 5 percent — not even for a minute.
I’ve given up on the commercial weight-loss circuit. It’s not that I don’t believe Weight Watchers, Jenny Craig and similar programs are beneficial. I’ve spent seven years as a WW member, but I’ve never had any long-term success with those types of programs.
I’ve worked with three dieticians in the past two years. They succeeded in helping me improve my food choices and figure out meal planning. One has even helped me make a healthier transition to a pseudo-vegetarian lifestyle (I now abstain from red meat and poultry).But we never succeeded in the realm of weight loss.
I have worked with a couple of therapists on my issues with emotional/binge eating and had great success. It’s been at least six months since I’ve binged, and I no longer use food to quell uncomfortable emotions. But I still haven’t lost much more than five or 10 pounds from changing those behaviors.
That’s where gastric-bypass surgery comes in. It’s a drastic solution, but I have a drastic problem.I thought about it for four months before talking with my primary physician. I had discussions with my husband — who was against it for some time — my mom — who remains opposed — and a handful of close friends and relatives — all of whom are cautiously supportive.
I’ve had to discuss my decision with loved ones because they have a right to know, my employer because I will need a significant amount of time off and my health-care providers because their opinions determine whether my insurance company will cover the procedure.
I spent four months poring over research and patient accounts of the different types of surgery available. I devoted at least two months investigating my insurer’s policy on weight-loss surgery.
It’s a good thing I did that, too. Though there are a handful of different styles of weight-loss surgery performed in the United States, my health-maintenance organization only covers one — the Roux-en-Y gastric bypass, which I’ll discuss further in next week’s column.Gathering information on the procedure was daunting.
Actually, that’s a lie. Gathering information was easy; gathering information that can be understood by the average person was a different story.
When I first discussed gastric bypass with my doctor, he sent me home with a 60-page booklet published by my insurer that made my college biology textbook seem engaging. It took me a week of hard concentrating to plow through it, and I’m typically a fast reader.
I found my most useful information on the Internet.
Sure, not everything on the Web is credible, but there is a plethora of sites created by weight-loss surgery patients. One thing I’ve discovered is that WLS patients are part of a warm, welcoming community. For the most part, they have worked very hard to be successful and they want to help others do the same. There are also numerous Internet message boards that freely disseminate information and advice. Message boards are great because they are interactive; you can post questions and have them answered quickly. Finding out everything I could about surgical weight loss was important to me.
I’m almost embarrassed to admit it now, but I’ve been a vocal opponent of weight-loss surgery for a long time.Like many people, I thought surgery was a lazy way out. I knew it would be hard for me to explain to my loved ones why my tune suddenly changed. And it was important to me that I could justify it to myself.
Research helped me change my mind rather quickly. The first thing I discovered is that gastric bypass is far from a passive method of weight loss. Most bypass patients report spending more time planning their meals and exercising than ever before.
What I think makes surgical weight loss so much more effective than other methods is the rapid weight loss. Surgery patients are able to drop weight fast enough that exercise becomes easier on their bodies — which motivates and enables them to stick with it.That quick weight loss also serves as an emotionally motivating factor. It’s easier to feel successful when you can see your body changing before your own eyes.
I only finally decided that surgery was the option for me about a month ago. I spent about eight months weighing my options (no pun intended) and telling myself that I should try traditional methods one last time.
I’ve come to accept that traditional methods haven’t worked for me, and it’s time to try something else. It’s not going to be easy, but I’m willing to go through this in the hopes of one day becoming a mother — and a healthy one at that.
I’m officially under the gun to lose weight. I have obesity-related infertility, and if my husband and I hope to conceive the old fashioned way, I need to drop at least 100 pounds. And my doctor suggests I do it sooner rather than later. That’s no easy undertaking.After all, only 5 percent of Americans who diet are successful at maintaining weight loss. I’ve never been among that 5 percent — not even for a minute.
I’ve given up on the commercial weight-loss circuit. It’s not that I don’t believe Weight Watchers, Jenny Craig and similar programs are beneficial. I’ve spent seven years as a WW member, but I’ve never had any long-term success with those types of programs.
I’ve worked with three dieticians in the past two years. They succeeded in helping me improve my food choices and figure out meal planning. One has even helped me make a healthier transition to a pseudo-vegetarian lifestyle (I now abstain from red meat and poultry).But we never succeeded in the realm of weight loss.
I have worked with a couple of therapists on my issues with emotional/binge eating and had great success. It’s been at least six months since I’ve binged, and I no longer use food to quell uncomfortable emotions. But I still haven’t lost much more than five or 10 pounds from changing those behaviors.
That’s where gastric-bypass surgery comes in. It’s a drastic solution, but I have a drastic problem.I thought about it for four months before talking with my primary physician. I had discussions with my husband — who was against it for some time — my mom — who remains opposed — and a handful of close friends and relatives — all of whom are cautiously supportive.
I’ve had to discuss my decision with loved ones because they have a right to know, my employer because I will need a significant amount of time off and my health-care providers because their opinions determine whether my insurance company will cover the procedure.
I spent four months poring over research and patient accounts of the different types of surgery available. I devoted at least two months investigating my insurer’s policy on weight-loss surgery.
It’s a good thing I did that, too. Though there are a handful of different styles of weight-loss surgery performed in the United States, my health-maintenance organization only covers one — the Roux-en-Y gastric bypass, which I’ll discuss further in next week’s column.Gathering information on the procedure was daunting.
Actually, that’s a lie. Gathering information was easy; gathering information that can be understood by the average person was a different story.
When I first discussed gastric bypass with my doctor, he sent me home with a 60-page booklet published by my insurer that made my college biology textbook seem engaging. It took me a week of hard concentrating to plow through it, and I’m typically a fast reader.
I found my most useful information on the Internet.
Sure, not everything on the Web is credible, but there is a plethora of sites created by weight-loss surgery patients. One thing I’ve discovered is that WLS patients are part of a warm, welcoming community. For the most part, they have worked very hard to be successful and they want to help others do the same. There are also numerous Internet message boards that freely disseminate information and advice. Message boards are great because they are interactive; you can post questions and have them answered quickly. Finding out everything I could about surgical weight loss was important to me.
I’m almost embarrassed to admit it now, but I’ve been a vocal opponent of weight-loss surgery for a long time.Like many people, I thought surgery was a lazy way out. I knew it would be hard for me to explain to my loved ones why my tune suddenly changed. And it was important to me that I could justify it to myself.
Research helped me change my mind rather quickly. The first thing I discovered is that gastric bypass is far from a passive method of weight loss. Most bypass patients report spending more time planning their meals and exercising than ever before.
What I think makes surgical weight loss so much more effective than other methods is the rapid weight loss. Surgery patients are able to drop weight fast enough that exercise becomes easier on their bodies — which motivates and enables them to stick with it.That quick weight loss also serves as an emotionally motivating factor. It’s easier to feel successful when you can see your body changing before your own eyes.
I only finally decided that surgery was the option for me about a month ago. I spent about eight months weighing my options (no pun intended) and telling myself that I should try traditional methods one last time.
I’ve come to accept that traditional methods haven’t worked for me, and it’s time to try something else. It’s not going to be easy, but I’m willing to go through this in the hopes of one day becoming a mother — and a healthy one at that.
Saturday, December 11, 2004
Drastic measures for drastic times

Originally published Dec. 11, 2004, in the Tracy Press.
Few souls would embark on a weight-loss plan in the middle of the holiday season.
Fewer still would do so publicly, as I’m about to do. My journey is different from many in that I’m opting for a drastic solution to my weight problem — gastric-bypass surgery. Contrary to the belief of some, including myself at first, deciding to go under the knife is not an easy choice to make. In fact, it’s the hardest decision I’ve ever made. But I’ve come to realize it’s the only choice I have.
For me, this isn’t about fitting into a certain size or looking good in a bikini. Two decades of obesity has ensured that I will never look good in a bathing suit. This is about my health. I have been overweight for as long as I can remember. My size was encouraged. I remember being praised by the school lunchroom attendant for always eating all of my food. The idea of “bigger is better” was ingrained in my family. I was praised when I gained weight or outgrew a size. I was a happy kid with a bulging belly and chunky thighs.
By the third grade, I weighed 111 pounds. It didn’t occur to me that anything was wrong with that until a teacher asked if I wanted her to remove my weight from the classroom biographical chart. I had no idea until I saw that chart that most of my classmates weighed 60 to 70 pounds. Of course, that’s about the time that playing tag and hide-and-seek stopped appealing to me. I preferred instead to read books during recess or trade Garbage Pail Kids cards with my friends. I was teased a lot, but those memories are vague. As an only child, I didn’t have any siblings to motivate me to be active, either. It was just me and my mom — who was overweight herself — keeping each other company. By the fifth grade, I was about 5 feet tall and weighed 199 pounds. That weight on a 21-year-old woman equates to a body mass index of 38 — or severely obese.
If my life has been a war with obesity, the fifth grade is when I first engaged in battle.
By this time, I understood that I looked different than other kids. I couldn’t buy the same clothes in the same stores as the cool kids, and keeping my ever-expanding body in clothes was an expensive endeavor at best. I made up my mind that I would not gain any more weight. I almost succeeded. I did fairly well maintaining my weight from fifth grade through high school, graduating at about 205 pounds.
I wish I could say the same about my college years. By the time I graduated from college, I had packed on another 100 pounds doing nothing in particular — though I’m sure my stints working in fast food and my own casual dining didn’t help. Five years later, I’ve added even more to my 5-foot, 4- inch frame. My body mass index, or BMI, is now 56, well above being morbidly obese.
According to the BMI chart on ObesityHelp, I’m “super obese.” Maybe I should buy a cape and some queen-size tights.
Any way you look at it, I’ve been severely obese for 20 years. The problem is that the consequences have finally begun to catch up with me. I have high blood pressure, bad knees, a bad hip and problems with fluid retention — and I’m only 27.
I’ve tried just about every diet and exercise program on the market, with minimal success.Even after trying — and failing — each program, I still didn’t feel like I had tried everything. I figured my failures were symptoms of a greater character flaw. I would tell myself that once I was truly fed up with the weight, I would find a method, stick to it and be able to be fit and healthy, once and for all.
That day of being fed up finally came earlier this year, though not in the way I expected. I imagined it would come after I had children and was frustrated with lugging around babies and “baby weight.” But instead it came in an OB/GYN’s office when I was diagnosed with obesity-r-elated infertility.That’s when my weight stopped being about me, and I realized how my battle with obesity affected those around me, particularly my husband and our future family.
Obesity-related infertility isn’t uncommon. Stored fat also holds stored estrogen, and when you have lots of stored fat, all that estrogen confuses your reproductive system.
Doctors can prescribe drugs to trick the body into ignoring the excess estrogen or force the body to ovulate. Or they can perform artificial insemination and fertilization procedures.
But to me, it just doesn’t make sense to combat this obesity-related hormone imbalance with more hormones. All of those prescriptions and procedures seem more like a Band-Aid than anything else.
After all, if getting my fertility back — if I ever had it to begin with — is as simple as losing weight, why not just solve the basic problem of obesity?
Few souls would embark on a weight-loss plan in the middle of the holiday season.
Fewer still would do so publicly, as I’m about to do. My journey is different from many in that I’m opting for a drastic solution to my weight problem — gastric-bypass surgery. Contrary to the belief of some, including myself at first, deciding to go under the knife is not an easy choice to make. In fact, it’s the hardest decision I’ve ever made. But I’ve come to realize it’s the only choice I have.
For me, this isn’t about fitting into a certain size or looking good in a bikini. Two decades of obesity has ensured that I will never look good in a bathing suit. This is about my health. I have been overweight for as long as I can remember. My size was encouraged. I remember being praised by the school lunchroom attendant for always eating all of my food. The idea of “bigger is better” was ingrained in my family. I was praised when I gained weight or outgrew a size. I was a happy kid with a bulging belly and chunky thighs.
By the third grade, I weighed 111 pounds. It didn’t occur to me that anything was wrong with that until a teacher asked if I wanted her to remove my weight from the classroom biographical chart. I had no idea until I saw that chart that most of my classmates weighed 60 to 70 pounds. Of course, that’s about the time that playing tag and hide-and-seek stopped appealing to me. I preferred instead to read books during recess or trade Garbage Pail Kids cards with my friends. I was teased a lot, but those memories are vague. As an only child, I didn’t have any siblings to motivate me to be active, either. It was just me and my mom — who was overweight herself — keeping each other company. By the fifth grade, I was about 5 feet tall and weighed 199 pounds. That weight on a 21-year-old woman equates to a body mass index of 38 — or severely obese.
If my life has been a war with obesity, the fifth grade is when I first engaged in battle.
By this time, I understood that I looked different than other kids. I couldn’t buy the same clothes in the same stores as the cool kids, and keeping my ever-expanding body in clothes was an expensive endeavor at best. I made up my mind that I would not gain any more weight. I almost succeeded. I did fairly well maintaining my weight from fifth grade through high school, graduating at about 205 pounds.
I wish I could say the same about my college years. By the time I graduated from college, I had packed on another 100 pounds doing nothing in particular — though I’m sure my stints working in fast food and my own casual dining didn’t help. Five years later, I’ve added even more to my 5-foot, 4- inch frame. My body mass index, or BMI, is now 56, well above being morbidly obese.
According to the BMI chart on ObesityHelp, I’m “super obese.” Maybe I should buy a cape and some queen-size tights.
Any way you look at it, I’ve been severely obese for 20 years. The problem is that the consequences have finally begun to catch up with me. I have high blood pressure, bad knees, a bad hip and problems with fluid retention — and I’m only 27.
I’ve tried just about every diet and exercise program on the market, with minimal success.Even after trying — and failing — each program, I still didn’t feel like I had tried everything. I figured my failures were symptoms of a greater character flaw. I would tell myself that once I was truly fed up with the weight, I would find a method, stick to it and be able to be fit and healthy, once and for all.
That day of being fed up finally came earlier this year, though not in the way I expected. I imagined it would come after I had children and was frustrated with lugging around babies and “baby weight.” But instead it came in an OB/GYN’s office when I was diagnosed with obesity-r-elated infertility.That’s when my weight stopped being about me, and I realized how my battle with obesity affected those around me, particularly my husband and our future family.
Obesity-related infertility isn’t uncommon. Stored fat also holds stored estrogen, and when you have lots of stored fat, all that estrogen confuses your reproductive system.
Doctors can prescribe drugs to trick the body into ignoring the excess estrogen or force the body to ovulate. Or they can perform artificial insemination and fertilization procedures.
But to me, it just doesn’t make sense to combat this obesity-related hormone imbalance with more hormones. All of those prescriptions and procedures seem more like a Band-Aid than anything else.
After all, if getting my fertility back — if I ever had it to begin with — is as simple as losing weight, why not just solve the basic problem of obesity?
Subscribe to:
Comments (Atom)