Originally published July 30, 2005, in Our Town for the Tracy Press.
I have begun to lose my hair. It’s not as dramatic as it sounds.As opposed to hair loss, I think a more accurate description is that I’m experiencing extreme thinning.I’ve been dreading this for about two months.Most doctors tell their patients that the hair-loss phase begins around 12 weeks after weight-loss surgery. However, most people I’ve talked to say it sets in between the fourth and fifth month. As for how long it lasts — well, opinions vary on that as well. I’ve heard everything from three to six months.But knowing that it was coming did nothing to ease the shock of it happening.
At first I just noticed that a few hairs would stick in my hands after I ran my fingers through my hair. Then I noticed that my pillow was covered in strands. But the most troubling experience was after washing my hair in the bathroom sink one morning.I generally wash my hair in the shower. But on this day, after rinsing my hair, my fingers were tangled with it.I looked in the sink, and if not for the color, I would have thought I had just finished washing the cat there. My chestnut-colored hair was matted in the drain and covered the sink’s porcelain.I was taken aback, but I think I handled it pretty well. I didn’t cry or act weird. I just rinsed off my hands, grabbed a wad of toilet tissue and wiped out the sink.I towel-dried my hair and took a long look in the mirror. No bald spots, no noticeable thin areas. In fact, if I didn’t know better, I would have thought my eyes were playing tricks on me.I credit preparation and perspective for helping me not to overreact to the situation. The preoperative classes I took helped prepare me for the inevitability of losing my hair. Some people naturally lose hair after major surgery. The trauma to the system is just too much for the fragile hair follicles.But with gastric-bypass patients, the body has to deal with a drastic reduction in nutrients, as well as massive weight loss — and those combine to make the follicles freak out and release hair.My awesome hair stylist helped me choose a short haircut that I love so that the thinning and regrowth would be less noticeable. I didn’t want to be one of those women with inch-long sprouts poking through shoulder-length hair.But perspective actually came after I noticed the hair loss.I was eating lunch with a friend and told her about this new development. She was concerned and asked how I was handling it. I told her that I was trying to keep a good attitude.To prove it, I said, “Wanna see something cool?” as I ran my fingers through my hair to show her all the loose strands that came out.“ Please don’t ever do that again,” she pleaded with a shudder. “It reminds me of my mom when she had chemo.”For a second, I stopped. Her mother was my godmother.I remember her bouts with cancer from the time we were in junior high until college. I remember seeing my godmother with no eyebrows and a wig. I remember seeing her with her natural hair again when we thought the cancer was gone. And I remember coming home on break to notice she was wearing a wig again.And that put me in my place. What I’m experiencing is insignificant compared to that.Yes, my hair is thinning. Yes, it’s disturbing. But I know it’s not a permanent affliction. I’ve been taking my vitamins and consuming protein so that my body has what it needs to regrow hair when the time is right. Until then, I will continue to sport the stylish haircut, and I’ll keep a lint brush handy to lift the strays from my clothing before leaving the house.And most people won’t even have a clue.
Saturday, July 30, 2005
Saturday, July 23, 2005
Changes from the inside out
Originally published July 23, 2005, in Our Town for the Tracy Press.
Before having gastric-bypass surgery, I felt aged beyond my years.When I decided on the option of surgical weight loss, I did it to improve my health, not because of vanity.Sure, the improvement in my appearance has been a welcome side effect. But I measure my success each day by how I feel.For most of the last five months, I’ve felt great. I feel as youthful as the calendar tells me I should.But for the last few weeks, I’ve noticed a couple of nagging pains. At first, it was just when driving. It took me a while to realize it. But when driving for more than a few minutes, I would get a strange numbness low in my back.I figured that it was time to adjust the car seat. I had been driving with it in the same position I did before surgery. I spent a week altering the seat position with no relief. Then I started waking up with my upper back hurting.“Now this is ridiculous,” I remember thinking when getting out of bed one morning.I remember telling myself before surgery that I was too young to feel as old as I did at the time. But it seemed like it was happening all over again. The aches and pains really started to annoy me, so much so that I considered seeing a doctor.Before scheduling an appointment, however, I decided to whine to my husband one day after work.It had been a long day, and I was beat. My lower back was numb from sitting at my desk without moving for so long.My upper back was hurting to the point that touching the flesh behind my shoulder would make me wince.My husband offered to rub my back in the hopes of relieving my discomfort. As he started on my lower back, the numbness began to dissipate.“Not so bad,” I thought. And I let him try the same thing to my shoulders.“Ow, not so hard, please,” I begged when he began. “Can you feel that knot?”My husband did not feel the knot. He decided to explore this pain of mine a bit further. His exploration consisted of pressing hard in certain areas while asking, “Does this hurt? How ’bout this?”My answers fluctuated between “no, not at all” and “If you do that one more time … .”Perplexed, my husband asked me to show him where I had the most pain. Feeling over my shoulder, I quickly pointed out the hard knot behind my right shoulder that had me so cranky.“Do you feel knots anywhere else”? he asked.Gingerly moving my fingers around the general area, I found that this knot of mine was much larger than I realized, and it seemed more inthe shape of a ridge.“Weird. Do you think it’s a growth of some sort”? the hypochondriac in me asked.My husband lightly ran his fingers over the same area.“This is the knot you’ve been complaining about”? he calmly asked. “Um, honey, that’s your shoulder blade. It’s supposedto be there.”I don’t know what my expression looked like, but I have to give the guy credit for not bursting into laughter. He then showed me how I had a similar ridge on the other side, and he assured me that many people share the same anatomical phenomenon without writhing in pain.Feeling like super-doc, my husband went in search of the source of my lower back pain.His diagnosis?“It’s a thing we like to call a ‘tail bone,’” he slowly explained, with all the sarcasm he could muster.At this point, I was incredulous. My husband is about 6- foot-5 and weighs all of 160 pounds soaking wet. Obviously, he has bones that jut out all over the place, and I’ve never heard him complain about them.He admits that he can’t figure out why sleeping on my back makes my shoulder blades hurt, but he knows exactly why my tail bone has been giving me trouble.“Why do you think I stop the car to walk around so much when we travel?” he asks.“Sitting for a long time really puts pressure there, and it doesn’t feel good.”His advice?“Don’t worry, babe. You’ll get used to it. Everyone does.”Thanks a lot.
Before having gastric-bypass surgery, I felt aged beyond my years.When I decided on the option of surgical weight loss, I did it to improve my health, not because of vanity.Sure, the improvement in my appearance has been a welcome side effect. But I measure my success each day by how I feel.For most of the last five months, I’ve felt great. I feel as youthful as the calendar tells me I should.But for the last few weeks, I’ve noticed a couple of nagging pains. At first, it was just when driving. It took me a while to realize it. But when driving for more than a few minutes, I would get a strange numbness low in my back.I figured that it was time to adjust the car seat. I had been driving with it in the same position I did before surgery. I spent a week altering the seat position with no relief. Then I started waking up with my upper back hurting.“Now this is ridiculous,” I remember thinking when getting out of bed one morning.I remember telling myself before surgery that I was too young to feel as old as I did at the time. But it seemed like it was happening all over again. The aches and pains really started to annoy me, so much so that I considered seeing a doctor.Before scheduling an appointment, however, I decided to whine to my husband one day after work.It had been a long day, and I was beat. My lower back was numb from sitting at my desk without moving for so long.My upper back was hurting to the point that touching the flesh behind my shoulder would make me wince.My husband offered to rub my back in the hopes of relieving my discomfort. As he started on my lower back, the numbness began to dissipate.“Not so bad,” I thought. And I let him try the same thing to my shoulders.“Ow, not so hard, please,” I begged when he began. “Can you feel that knot?”My husband did not feel the knot. He decided to explore this pain of mine a bit further. His exploration consisted of pressing hard in certain areas while asking, “Does this hurt? How ’bout this?”My answers fluctuated between “no, not at all” and “If you do that one more time … .”Perplexed, my husband asked me to show him where I had the most pain. Feeling over my shoulder, I quickly pointed out the hard knot behind my right shoulder that had me so cranky.“Do you feel knots anywhere else”? he asked.Gingerly moving my fingers around the general area, I found that this knot of mine was much larger than I realized, and it seemed more inthe shape of a ridge.“Weird. Do you think it’s a growth of some sort”? the hypochondriac in me asked.My husband lightly ran his fingers over the same area.“This is the knot you’ve been complaining about”? he calmly asked. “Um, honey, that’s your shoulder blade. It’s supposedto be there.”I don’t know what my expression looked like, but I have to give the guy credit for not bursting into laughter. He then showed me how I had a similar ridge on the other side, and he assured me that many people share the same anatomical phenomenon without writhing in pain.Feeling like super-doc, my husband went in search of the source of my lower back pain.His diagnosis?“It’s a thing we like to call a ‘tail bone,’” he slowly explained, with all the sarcasm he could muster.At this point, I was incredulous. My husband is about 6- foot-5 and weighs all of 160 pounds soaking wet. Obviously, he has bones that jut out all over the place, and I’ve never heard him complain about them.He admits that he can’t figure out why sleeping on my back makes my shoulder blades hurt, but he knows exactly why my tail bone has been giving me trouble.“Why do you think I stop the car to walk around so much when we travel?” he asks.“Sitting for a long time really puts pressure there, and it doesn’t feel good.”His advice?“Don’t worry, babe. You’ll get used to it. Everyone does.”Thanks a lot.
Saturday, July 16, 2005
Meaning well matters most
Originally published July 16, 2005, in Our Town for the Tracy Press.
Compliments are meant to be a good thing. The idea of a compliment is to make someone feel good about him or herself.
We’ve all run into people who aren’t very good at accepting compliments. They don’t realize that a simple “thank you” is the best response in all cases. However, since having gastric-bypass surgery, I’ve also run into an entirely different population — people who aren’t very good at giving compliments.
For the most part, I receive positive comments. “You look fabulous,” “You look amazing,” and “Wow! I can’t believe how much you’ve changed,” are among the comments I’ve heard that give me immediate warm fuzzies. And then there are the ones that don’t.
My sister-in-law is an example of someone who tends to stick her foot in her mouth when complimenting others.She loves me, and I know she’s proud of me. But that doesn’t stop me from wincing when she sees me and says, “Wow, Tonya. You’re starting to look really good.” Ouch. The first thought that comes to mind is, “Gee, how bad did I look before?” Then I remind myself that she’s sincere and she means well. And that’s when I smile and reply, “Thank you. That means a lot to me.” That’s not a lie, either. I know that coming from her, that’s a really big compliment.
Unfortunately, she made the mistake of saying the same thing last weekend in front of her brother. My husband didn’t take the compliment as graciously as I did. Instead, he said, “Starting to? I think she’s always looked good.”
Trying to play interference, I told her that he’s sensitive to compliments that imply I didn’t look good before. Of course, she tried to backpedal, but everything just sounded worse.The best one was, “I just meant that you’re starting to slim down.” I wanted to say, “So the first 50 pounds I lost made no difference? I must have looked really bad.” But I opted instead to say, “I know exactly what you mean, and I appreciate that you notice.”
Someone asked me last week about the type of comments I’ve received since having gastric-bypass surgery. He wanted to know whether I run into people who notice that I’ve changed but can’t seem to put their finger on how.The answer is that I have. Aside from writing this column, I don’t walk around announcing to the world that I’ve had weight-loss surgery. And though I wish it weren’t true, there are a few people in this town who don’t regularly read the Tracy Press. That combination makes for a decent-sized local population that doesn’t know I’ve had gastric bypass.And it’s those people — like my favorite checker at the grocery store, or the night-shift worker at the convenience store I usually visit during the day — who notice a change in me but aren’t sure what has changed.It doesn’t bother me that they don’t notice I’ve lost weight. I don’t make it a point to tell them about my weight loss, either.
Yes, I’ve lost 100 pounds, and that’s a big accomplishment for me. But I didn’t have gastric-bypass surgery just so people would notice. Sure, I love compliments and probably will never tire of people passing them on. But I did this for reasons other than attention, most of which pertain to my health. Those are changes that can’t be seen by others, but they are the ones that matter most.
Compliments are meant to be a good thing. The idea of a compliment is to make someone feel good about him or herself.
We’ve all run into people who aren’t very good at accepting compliments. They don’t realize that a simple “thank you” is the best response in all cases. However, since having gastric-bypass surgery, I’ve also run into an entirely different population — people who aren’t very good at giving compliments.
For the most part, I receive positive comments. “You look fabulous,” “You look amazing,” and “Wow! I can’t believe how much you’ve changed,” are among the comments I’ve heard that give me immediate warm fuzzies. And then there are the ones that don’t.
My sister-in-law is an example of someone who tends to stick her foot in her mouth when complimenting others.She loves me, and I know she’s proud of me. But that doesn’t stop me from wincing when she sees me and says, “Wow, Tonya. You’re starting to look really good.” Ouch. The first thought that comes to mind is, “Gee, how bad did I look before?” Then I remind myself that she’s sincere and she means well. And that’s when I smile and reply, “Thank you. That means a lot to me.” That’s not a lie, either. I know that coming from her, that’s a really big compliment.
Unfortunately, she made the mistake of saying the same thing last weekend in front of her brother. My husband didn’t take the compliment as graciously as I did. Instead, he said, “Starting to? I think she’s always looked good.”
Trying to play interference, I told her that he’s sensitive to compliments that imply I didn’t look good before. Of course, she tried to backpedal, but everything just sounded worse.The best one was, “I just meant that you’re starting to slim down.” I wanted to say, “So the first 50 pounds I lost made no difference? I must have looked really bad.” But I opted instead to say, “I know exactly what you mean, and I appreciate that you notice.”
Someone asked me last week about the type of comments I’ve received since having gastric-bypass surgery. He wanted to know whether I run into people who notice that I’ve changed but can’t seem to put their finger on how.The answer is that I have. Aside from writing this column, I don’t walk around announcing to the world that I’ve had weight-loss surgery. And though I wish it weren’t true, there are a few people in this town who don’t regularly read the Tracy Press. That combination makes for a decent-sized local population that doesn’t know I’ve had gastric bypass.And it’s those people — like my favorite checker at the grocery store, or the night-shift worker at the convenience store I usually visit during the day — who notice a change in me but aren’t sure what has changed.It doesn’t bother me that they don’t notice I’ve lost weight. I don’t make it a point to tell them about my weight loss, either.
Yes, I’ve lost 100 pounds, and that’s a big accomplishment for me. But I didn’t have gastric-bypass surgery just so people would notice. Sure, I love compliments and probably will never tire of people passing them on. But I did this for reasons other than attention, most of which pertain to my health. Those are changes that can’t be seen by others, but they are the ones that matter most.
Saturday, July 09, 2005
No such thing as perfection
Originally published July 9, 2005, in Our Town for the Tracy Press.
It’s been about 4½ months since I had gastric-bypass surgery, and I have a confession to make: I’m not perfect.Sure, you might say that nobody is perfect and that it’s no big deal. But when it comes to weight loss, I think a lot of us obsess with being perfect. And I also think that’s why most diets fail.
When dieting, many of us classify our behavior as “good” or “bad.” If we order the grilled-chicken salad with fat-free dressing (on the side, of course), we’re good. But if we instead choose the fried-chicken salad with ranch, or — heaven forbid — order dessert, we label ourselves as being bad.Often, one “bad” meal is blamed for throwing us off the wagon, and we end up on a bender of sorts. We stop watching our portions, we skip the gym, we stop asking for nonfat milk in our morning lattes. After all, if we were bad at lunch on Monday, how could we ever make up for it?With weight-loss surgery, perfectionism is moot. Everyone has a different experience with gastric bypass. And depending on where surgery is performed, rules for each patient may vary as well. But that doesn’t mean that the perfectionist attitude is miraculously removed during surgery. If anything, I think it can be made worse.
Within the WLS community, perfectionism is pervasive.On online message boards, I’ve seen people be chastised for eating a slice of pizza or carbohydrates or desserts. It’s not because people who’ve had surgery are mean. If anything, the WLS community is filled with people who take it upon themselves to help others on the same journey. But that also means that they can take it a little personally when they hear of someone eating things they think should be off-limits.
For example, before I had surgery, doctors drilled into my head that I should stay away from rice and pasta forever. But I know other patients who had doctors tell them pasta would be fine after three months, and rice would be allowed after six.I hear some of these patients telling me about trying rice and getting sick, and I cringe inside. After sitting through numerous nutrition classes, I can’t imagine why on earth any bypass patient would even try rice. But I don’t say anything, because I know there are others out there who have no trouble tolerating it.
And whenever I catch myself feeling superior to other bypass patients, which isn’t often, I remind myself that I do things that others wouldn’t approve of as well.
So, here are my confessions:
I don’t exercise enoughI’m really good about exercising twice a week, whether it’s at home or at the gym. And I make sure I keep active on the weekend, even if it’s just walking quickly around the mall. But my doctors want me exercising at least an hour a day, six days a week. Since surgery, I’ve met that goal for a total of three weeks.
I’m terrible about taking my vitaminsI don’t know when it happened, but I’ve fallen off the wagon with my vitamins. I think I might have taken an iron pill last week, but I don’t really remember. This came to mind over this weekend because I discovered a batch of nasty bruises appearing all over.
I eat too fastEating too fast leads to eating too much, and that could stretch out my pouch. Eating slowly is the hardest thing for me to do. But I work very hard to pay attention when eating. I also pay attention to how I feel after eating. If I feel particularly good after a meal, I’ll make note of what I ate, how long I spent eating and approximately how much I ate. And I’ll try to mimic that experience again. If I feel bad after eating, I’ll take the same notes.
I have tested my boundariesI have tried — and liked — Domino’s crispy thin-crust pizza. I have enjoyed a glass of white wine a few times since surgery. I have tried a bite of cookie and tiramisu. And I’m not sorry about it one bit. I’ve been very careful not to overindulge in sweets — my Achilles’ heel before surgery — and I realize that every time I try something with sugar in it, I could have a bad reaction. But I fear discovering that sugar doesn’t bother me at all and feeling able to eat as much as I want.
I don’t confess these things to garner sympathy or support. I do so because I think it’s important to point out that we are all human. Having gastric-bypass surgery did not give me superhuman willpower. All it has done is provide me with a little more strength. As I’ve said many times, it’s only a tool, not a cure.
It’s been about 4½ months since I had gastric-bypass surgery, and I have a confession to make: I’m not perfect.Sure, you might say that nobody is perfect and that it’s no big deal. But when it comes to weight loss, I think a lot of us obsess with being perfect. And I also think that’s why most diets fail.
When dieting, many of us classify our behavior as “good” or “bad.” If we order the grilled-chicken salad with fat-free dressing (on the side, of course), we’re good. But if we instead choose the fried-chicken salad with ranch, or — heaven forbid — order dessert, we label ourselves as being bad.Often, one “bad” meal is blamed for throwing us off the wagon, and we end up on a bender of sorts. We stop watching our portions, we skip the gym, we stop asking for nonfat milk in our morning lattes. After all, if we were bad at lunch on Monday, how could we ever make up for it?With weight-loss surgery, perfectionism is moot. Everyone has a different experience with gastric bypass. And depending on where surgery is performed, rules for each patient may vary as well. But that doesn’t mean that the perfectionist attitude is miraculously removed during surgery. If anything, I think it can be made worse.
Within the WLS community, perfectionism is pervasive.On online message boards, I’ve seen people be chastised for eating a slice of pizza or carbohydrates or desserts. It’s not because people who’ve had surgery are mean. If anything, the WLS community is filled with people who take it upon themselves to help others on the same journey. But that also means that they can take it a little personally when they hear of someone eating things they think should be off-limits.
For example, before I had surgery, doctors drilled into my head that I should stay away from rice and pasta forever. But I know other patients who had doctors tell them pasta would be fine after three months, and rice would be allowed after six.I hear some of these patients telling me about trying rice and getting sick, and I cringe inside. After sitting through numerous nutrition classes, I can’t imagine why on earth any bypass patient would even try rice. But I don’t say anything, because I know there are others out there who have no trouble tolerating it.
And whenever I catch myself feeling superior to other bypass patients, which isn’t often, I remind myself that I do things that others wouldn’t approve of as well.
So, here are my confessions:
I don’t exercise enoughI’m really good about exercising twice a week, whether it’s at home or at the gym. And I make sure I keep active on the weekend, even if it’s just walking quickly around the mall. But my doctors want me exercising at least an hour a day, six days a week. Since surgery, I’ve met that goal for a total of three weeks.
I’m terrible about taking my vitaminsI don’t know when it happened, but I’ve fallen off the wagon with my vitamins. I think I might have taken an iron pill last week, but I don’t really remember. This came to mind over this weekend because I discovered a batch of nasty bruises appearing all over.
I eat too fastEating too fast leads to eating too much, and that could stretch out my pouch. Eating slowly is the hardest thing for me to do. But I work very hard to pay attention when eating. I also pay attention to how I feel after eating. If I feel particularly good after a meal, I’ll make note of what I ate, how long I spent eating and approximately how much I ate. And I’ll try to mimic that experience again. If I feel bad after eating, I’ll take the same notes.
I have tested my boundariesI have tried — and liked — Domino’s crispy thin-crust pizza. I have enjoyed a glass of white wine a few times since surgery. I have tried a bite of cookie and tiramisu. And I’m not sorry about it one bit. I’ve been very careful not to overindulge in sweets — my Achilles’ heel before surgery — and I realize that every time I try something with sugar in it, I could have a bad reaction. But I fear discovering that sugar doesn’t bother me at all and feeling able to eat as much as I want.
I don’t confess these things to garner sympathy or support. I do so because I think it’s important to point out that we are all human. Having gastric-bypass surgery did not give me superhuman willpower. All it has done is provide me with a little more strength. As I’ve said many times, it’s only a tool, not a cure.
Saturday, July 02, 2005
The hidden price of weight loss
Originally published July 2, 2005, in Our Town for the Tracy Press.
Losing weight is expensive, regardless of the method used.Eating less might mean fewer groceries purchased at the store, but eating healthier often means those few groceries cost a lot more as well. And then there are the hidden costs that seem to creep up without notice — like a new wardrobe.This is especially true for gastric-bypass patients. After surgery, the grocery-store bill might drop anywhere from $200 to $400 a trip, depending on the size of the patient’s family. But for most people who’ve had weight loss surgery, the grocery store isn’t the only place to buy food.
Sugar-free protein supplement bars and powders are often bought from specialty stores and Web sites — and they don’t come cheap.Zero Carb Isopure is a popular supplement powder among gastric-bypass patients. A 3-pound canister of the powder is about $40 at MuscleGear on 11th Street. There are 44 scoops of powder in each container, which is enough for 22 days of supplementation for gastric-bypass patients.
Spending $1.82 for breakfast or lunch every day is pretty frugal, but few patients have just one method of supplementation. It’s common for those who’ve had surgery to keep a variety of powders and supplement bars in supply.
Vitamins are another necessity for anyone who has had bariatric surgery. Prices depend largely on the brand chosen.VistaVitamins, created specifically for bariatric patients, costs about $50 a month, not including calcium supplementation. Calcium supplements add another $20 or $30 each month.Vitamins from Bariatric Advantage, which are all chewable, cost around $60 a month for everything from multivitamins to iron to B-12 to calcium. Either way, that’s another $60 to $80 to add to the grocery bill.
Surgical weight-loss patients who are serious about achieving long-term success consider gym memberships and personal-training appointments as necessities rather than luxuries — and their doctors often agree.
Gym memberships in this town are pretty cheap, about $40 a month. Personal training is billed by the hour —about $400 a month.Suddenly, all that money saved at the grocery store — and then some — is missing from the checking account.
Still, it’s the hidden costs that are more surprising. Though most doctors repeatedly tell patients that they will experience rapid weight loss, it doesn’t always hit home until it becomes a reality.Losing an average of 10 to 20 pounds a month means a new wardrobe about every six weeks. Life goes along swimmingly while one is shopping in one’s closet. But eventually, the closet runs out of smaller sizes, or at least clothes that are still in style, and a shopping excursion is necessary.
Shopping trips must be well planned, because it’s easy to get excited about being a size smaller and overspend. Sales and clearances must be the first stop. After all, a similar shopping trip will be needed in a few weeks for even smaller clothes. Everything must be tried on with the question, “Is this loose enough to be presentable in public but tight enough to last at least a month?”
Then there is the checkout, which, if the shopper is lucky, will end with a total under three figures.Other hidden costs often are attributed to newfound addictions. For example, a new love of sandals might necessitate regular pedicure appointments all summer long.
The desire to leave the house looking as good as possible each day might mean more money spent at the salon and makeup counter, too.However, there aren’t many people who choose surgical weight loss in the hopes of saving money. The fact is that, regardless of the costs associated with rapid weight loss, the benefits are immeasurable.
Losing weight is expensive, regardless of the method used.Eating less might mean fewer groceries purchased at the store, but eating healthier often means those few groceries cost a lot more as well. And then there are the hidden costs that seem to creep up without notice — like a new wardrobe.This is especially true for gastric-bypass patients. After surgery, the grocery-store bill might drop anywhere from $200 to $400 a trip, depending on the size of the patient’s family. But for most people who’ve had weight loss surgery, the grocery store isn’t the only place to buy food.
Sugar-free protein supplement bars and powders are often bought from specialty stores and Web sites — and they don’t come cheap.Zero Carb Isopure is a popular supplement powder among gastric-bypass patients. A 3-pound canister of the powder is about $40 at MuscleGear on 11th Street. There are 44 scoops of powder in each container, which is enough for 22 days of supplementation for gastric-bypass patients.
Spending $1.82 for breakfast or lunch every day is pretty frugal, but few patients have just one method of supplementation. It’s common for those who’ve had surgery to keep a variety of powders and supplement bars in supply.
Vitamins are another necessity for anyone who has had bariatric surgery. Prices depend largely on the brand chosen.VistaVitamins, created specifically for bariatric patients, costs about $50 a month, not including calcium supplementation. Calcium supplements add another $20 or $30 each month.Vitamins from Bariatric Advantage, which are all chewable, cost around $60 a month for everything from multivitamins to iron to B-12 to calcium. Either way, that’s another $60 to $80 to add to the grocery bill.
Surgical weight-loss patients who are serious about achieving long-term success consider gym memberships and personal-training appointments as necessities rather than luxuries — and their doctors often agree.
Gym memberships in this town are pretty cheap, about $40 a month. Personal training is billed by the hour —about $400 a month.Suddenly, all that money saved at the grocery store — and then some — is missing from the checking account.
Still, it’s the hidden costs that are more surprising. Though most doctors repeatedly tell patients that they will experience rapid weight loss, it doesn’t always hit home until it becomes a reality.Losing an average of 10 to 20 pounds a month means a new wardrobe about every six weeks. Life goes along swimmingly while one is shopping in one’s closet. But eventually, the closet runs out of smaller sizes, or at least clothes that are still in style, and a shopping excursion is necessary.
Shopping trips must be well planned, because it’s easy to get excited about being a size smaller and overspend. Sales and clearances must be the first stop. After all, a similar shopping trip will be needed in a few weeks for even smaller clothes. Everything must be tried on with the question, “Is this loose enough to be presentable in public but tight enough to last at least a month?”
Then there is the checkout, which, if the shopper is lucky, will end with a total under three figures.Other hidden costs often are attributed to newfound addictions. For example, a new love of sandals might necessitate regular pedicure appointments all summer long.
The desire to leave the house looking as good as possible each day might mean more money spent at the salon and makeup counter, too.However, there aren’t many people who choose surgical weight loss in the hopes of saving money. The fact is that, regardless of the costs associated with rapid weight loss, the benefits are immeasurable.
Saturday, June 25, 2005
‘Morbidly obese’ means progress
Originally published June 25, 2005, in Our Town for the Tracy Press.
It’s been four months since I had gastric-bypass surgery, and life just keeps improving.
I’ve lost about 74 pounds — 100 pounds since my highest weight last summer — and the sense of accomplishment is almost indescribable.
As I’ve mentioned in previous columns, I was never able to lose more than about 30 pounds with other weight loss methods. Though I knew that gastric bypass boasts a 95 percent success rate, in the back of my mind, I thought I would be among the 5 percent for whom it didn’t work.
Instead, I’m amazed every week I step on the scale. I’ve gone from a body-mass index, BMI, of near 60 — considered “super obese” — to 41.6 — the low end of the no-less-scary “morbidly obese” distinction.The BMI is a number often thrown around by health-care and fitness professionals to determine whether a person’s weight is healthy for his or her height. I had originally reported my BMI in this column as being 56 before I had surgery.
Unfortunately, that was at a time when I thought I was taller than I really am.
The funny thing is that even after losing a total of 100 pounds, my BMI is still high enough to qualify me for surgical weight loss and have the procedure covered by most insurers. Talk about putting things in perspective.
I continue to be amazed by people’s reactions to me. A woman at the gym the other day told me I looked like my sister. Not that I have a sister, but she said my features have changed so much that I look like a relative of my former self.
I get asked a lot if I’m considered a success. I generally say that success is relative. If I had dropped 100 pounds through standard diet and exercise modifications, my physician wouldn’t mind if I chose to stop losing weight right now. After all, anything is better than where I was before, and maintenance is the hardest part of weight control.
Having gastric-bypass surgery changes that perspective.Doctors have varying opinions on what constitutes success with this surgery. Most insurers are happy if a patient loses 50 percent of his or her excess weight. But some doctors set higher goals to put a patient’s BMI closer to the “normal” range. The accepted average is that surgical weight loss can help patients lose about 65 percent of their excess weight.
I’m on track to lose 75 percent of the extra weight I carried at the time of surgery.
Because I am 5-feet-3-inches tall, insurance charts say I should weigh 130. Rounding my pre-surgery weight down to 309 pounds, that means I’m on track to weigh 175 pounds after 18 months, for a total loss of 134 pounds. That gives me 14 more months to drop 60 pounds.
Chances are, I’ll lose more than that over the next year, but at least I have an idea of the weight at which my body may decide to rest. And I hope that knowledge prevents me from obsessing over the fact that 175 pounds on a 5-foot-3-inch frame is still considered obese.
It’s been four months since I had gastric-bypass surgery, and life just keeps improving.
I’ve lost about 74 pounds — 100 pounds since my highest weight last summer — and the sense of accomplishment is almost indescribable.
As I’ve mentioned in previous columns, I was never able to lose more than about 30 pounds with other weight loss methods. Though I knew that gastric bypass boasts a 95 percent success rate, in the back of my mind, I thought I would be among the 5 percent for whom it didn’t work.
Instead, I’m amazed every week I step on the scale. I’ve gone from a body-mass index, BMI, of near 60 — considered “super obese” — to 41.6 — the low end of the no-less-scary “morbidly obese” distinction.The BMI is a number often thrown around by health-care and fitness professionals to determine whether a person’s weight is healthy for his or her height. I had originally reported my BMI in this column as being 56 before I had surgery.
Unfortunately, that was at a time when I thought I was taller than I really am.
The funny thing is that even after losing a total of 100 pounds, my BMI is still high enough to qualify me for surgical weight loss and have the procedure covered by most insurers. Talk about putting things in perspective.
I continue to be amazed by people’s reactions to me. A woman at the gym the other day told me I looked like my sister. Not that I have a sister, but she said my features have changed so much that I look like a relative of my former self.
I get asked a lot if I’m considered a success. I generally say that success is relative. If I had dropped 100 pounds through standard diet and exercise modifications, my physician wouldn’t mind if I chose to stop losing weight right now. After all, anything is better than where I was before, and maintenance is the hardest part of weight control.
Having gastric-bypass surgery changes that perspective.Doctors have varying opinions on what constitutes success with this surgery. Most insurers are happy if a patient loses 50 percent of his or her excess weight. But some doctors set higher goals to put a patient’s BMI closer to the “normal” range. The accepted average is that surgical weight loss can help patients lose about 65 percent of their excess weight.
I’m on track to lose 75 percent of the extra weight I carried at the time of surgery.
Because I am 5-feet-3-inches tall, insurance charts say I should weigh 130. Rounding my pre-surgery weight down to 309 pounds, that means I’m on track to weigh 175 pounds after 18 months, for a total loss of 134 pounds. That gives me 14 more months to drop 60 pounds.
Chances are, I’ll lose more than that over the next year, but at least I have an idea of the weight at which my body may decide to rest. And I hope that knowledge prevents me from obsessing over the fact that 175 pounds on a 5-foot-3-inch frame is still considered obese.
Saturday, June 18, 2005
Feeling reformed
Originally published June 18, 2005, in Our Town for the Tracy Press.
Exercise can be a tedious chore. That’s probably why so many Americans don’t do much of it. In bigger cities, health clubs recognize this and try to offer unusual options to attract members. Spinning, kick boxing and even stripper-cise are all examples of recent fitness trends that professionals have tried to cash in on.
I started doing yoga when the most-recent craze hit town about five years ago, and for two years, I was a yoga fanatic — who knew you could get such a great workout by breathing and stretching?
Classes have never been my thing. I always find that I’m the least coordinated or fit person in the class, and I rarely have the stamina to make it to the end. But when I was in my yoga craze, I craved more instruction. I tried every class related to yoga offered by my gym — cardio yoga, power yoga and even something called Pilates.
Sadly, the experience wasn’t as rewarding as I hoped. The yoga craze had created a monster, and most of the hybrid classes weren’t really yoga at all, at least not the type of yoga I learned and was growing to love.
I had been told Pilates was the same as yoga, only it focused more on the core muscles of the abdomen and back. I didn’t have any luck in the Pilates class either. The moves were very difficult and fast. I tried the classes twice a week. But after a month of leaving with a sore neck and back, I gave up and figured I was just too big to do it.
It wasn’t until I started reading more about Pilates that I realized that the instructor I had wasn’t teaching true Pilates. Created by Joseph Pilates, a performer and boxer in the early 1900s, the exercise form has been widely used by dancers. His goal was to give people who were injured the ability to exercise their muscles. Pilates incorporates controlled breathing with controlled movements to offer a total-body strengthening workout with minimal risk of injury.
Part of the reason the risk of injury is low is that Joseph Pilates also invented an array of contraptions to help people do his exercises correctly and safely.
When I was preparing to have gastric-bypass surgery, I picked up a Pilates DVD. Many gastric-bypass patients swear by Pilates. Patients who have open procedures (a 4- to 7-inch midline incision) aren’t usually allowed to do standard abdominal exercises, because they are at risk of incisional hernias. Pilates is a way to exercise their abs and back without injuring themselves.
Though I could tell the instructor on the DVD knew what she was doing, I still had difficulty. Controlled breathing is very important in Pilates. It’s so important that if you can’t breathe properly, there’s really no benefit to doing the exercises.
My problem with the DVD was that if I was concentrating on my breathing, I couldn’t figure out the moves. But if I concentrated on my movement, I couldn’t maintain the breathing. I turned off the video and shelved what I figured would be another $20 down the drain.Fast forward four months. Bored with my exercise routine, I started to feel that no matter how much I was exercising, my fitness level was dropping.
I decided it was time to visit my personal trainer to see if she could help me rework my routine.She asked me if I wanted to try something called the Reformer. The Reformer is an exercise machines invented by Joseph Pilates.Apparently, the gym had recently bought one, and the trainer was eager to use it. I looked at it, gulped and told her I would. To be truthful, I wanted to say no. The machine looked like a medieval torture device. But just recently I wrote a column about wanting more adventure, and the Reformer seemed like a good place to start.We started by taking off our shoes, and the trainer showed me how the machine worked.
Joseph Pilates constructed the original Reformer by taking apart a hospital bed. The platform glides back and forth. Springs attached to the base govern the resistance provided for each exercise. There are a variety of straps and pulleys that attach to the springs as well.At first, I just sat on the platform to get a feel for its movement. Once I was comfortable with that, I laid on the platform, and my trainer coached me through Pilates breathing. The breathing technique can be difficult to master. It involves pulling in your navel toward your spine and breathing into your lower belly.
Once I seemed to have a grasp on that, and keeping my spine in a neutral position, I actually started doing some exercises. The exercises were difficult because of the level of control needed to perform them as slowly as the Pilates method demands. When breathing correctly, I would be dripping with sweat. When my body began to cool, I realized that I needed to correct my breathing.
After the workout, I was spent. I’m sure to those around me, it didn’t look like I did much. But I felt it for six days. It was truly an Abs of Steel workout.
Since the exercise session, I have become like a convert, preaching the Gospel to the world. I tell everyone that Pilates done right is the best workout around. It’s a mental and physical challenge that leaves you feeling rejuvenated and exhausted all at the same time.
Exercise can be a tedious chore. That’s probably why so many Americans don’t do much of it. In bigger cities, health clubs recognize this and try to offer unusual options to attract members. Spinning, kick boxing and even stripper-cise are all examples of recent fitness trends that professionals have tried to cash in on.
I started doing yoga when the most-recent craze hit town about five years ago, and for two years, I was a yoga fanatic — who knew you could get such a great workout by breathing and stretching?
Classes have never been my thing. I always find that I’m the least coordinated or fit person in the class, and I rarely have the stamina to make it to the end. But when I was in my yoga craze, I craved more instruction. I tried every class related to yoga offered by my gym — cardio yoga, power yoga and even something called Pilates.
Sadly, the experience wasn’t as rewarding as I hoped. The yoga craze had created a monster, and most of the hybrid classes weren’t really yoga at all, at least not the type of yoga I learned and was growing to love.
I had been told Pilates was the same as yoga, only it focused more on the core muscles of the abdomen and back. I didn’t have any luck in the Pilates class either. The moves were very difficult and fast. I tried the classes twice a week. But after a month of leaving with a sore neck and back, I gave up and figured I was just too big to do it.
It wasn’t until I started reading more about Pilates that I realized that the instructor I had wasn’t teaching true Pilates. Created by Joseph Pilates, a performer and boxer in the early 1900s, the exercise form has been widely used by dancers. His goal was to give people who were injured the ability to exercise their muscles. Pilates incorporates controlled breathing with controlled movements to offer a total-body strengthening workout with minimal risk of injury.
Part of the reason the risk of injury is low is that Joseph Pilates also invented an array of contraptions to help people do his exercises correctly and safely.
When I was preparing to have gastric-bypass surgery, I picked up a Pilates DVD. Many gastric-bypass patients swear by Pilates. Patients who have open procedures (a 4- to 7-inch midline incision) aren’t usually allowed to do standard abdominal exercises, because they are at risk of incisional hernias. Pilates is a way to exercise their abs and back without injuring themselves.
Though I could tell the instructor on the DVD knew what she was doing, I still had difficulty. Controlled breathing is very important in Pilates. It’s so important that if you can’t breathe properly, there’s really no benefit to doing the exercises.
My problem with the DVD was that if I was concentrating on my breathing, I couldn’t figure out the moves. But if I concentrated on my movement, I couldn’t maintain the breathing. I turned off the video and shelved what I figured would be another $20 down the drain.Fast forward four months. Bored with my exercise routine, I started to feel that no matter how much I was exercising, my fitness level was dropping.
I decided it was time to visit my personal trainer to see if she could help me rework my routine.She asked me if I wanted to try something called the Reformer. The Reformer is an exercise machines invented by Joseph Pilates.Apparently, the gym had recently bought one, and the trainer was eager to use it. I looked at it, gulped and told her I would. To be truthful, I wanted to say no. The machine looked like a medieval torture device. But just recently I wrote a column about wanting more adventure, and the Reformer seemed like a good place to start.We started by taking off our shoes, and the trainer showed me how the machine worked.
Joseph Pilates constructed the original Reformer by taking apart a hospital bed. The platform glides back and forth. Springs attached to the base govern the resistance provided for each exercise. There are a variety of straps and pulleys that attach to the springs as well.At first, I just sat on the platform to get a feel for its movement. Once I was comfortable with that, I laid on the platform, and my trainer coached me through Pilates breathing. The breathing technique can be difficult to master. It involves pulling in your navel toward your spine and breathing into your lower belly.
Once I seemed to have a grasp on that, and keeping my spine in a neutral position, I actually started doing some exercises. The exercises were difficult because of the level of control needed to perform them as slowly as the Pilates method demands. When breathing correctly, I would be dripping with sweat. When my body began to cool, I realized that I needed to correct my breathing.
After the workout, I was spent. I’m sure to those around me, it didn’t look like I did much. But I felt it for six days. It was truly an Abs of Steel workout.
Since the exercise session, I have become like a convert, preaching the Gospel to the world. I tell everyone that Pilates done right is the best workout around. It’s a mental and physical challenge that leaves you feeling rejuvenated and exhausted all at the same time.
Saturday, June 11, 2005
Adjusting to a whole new world
Originally published June 11, 2005, in Our Town for the Tracy Press.
Before having gastric-bypass surgery, I loathed placing myself in the category of being overweight. I considered myself more active and more nutritionally educated than most of my peers, obese or not. I also thought I had more confidence than other women. I had a husband who never complained and thought I was gorgeous. I paid attention to my appearance and tried my best not to be slovenly.
Of course, the bigger I got, the less those things seemed important or even possible and the more I saw myself as a hopelessly obese person. I felt that there was no point trying to improve myself because it wasn’t possible or even worth the trouble.
Taking the elevator to my second-floor office became more of a necessity than an example of laziness. My knees just couldn’t handle lugging all 300-plus pounds of me up a single flight of stairs. Even getting out of my office chair to walk across the room to the printer seemed an impossible feat.
At home, things were no better. I stopped painting my toenails because I couldn’t reach my feet. Shaving my legs stopped being an absentminded shower habit and started requiring advanced planning. When would I have time to lock myself in the bathroom for hours as I tried to contort myself to reach hairy patches of skin with a sharp blade? To be truthful, I lost the energy to even think about shaving.
While others spent their weekends planning hiking, skiing or boating trips, I preferred to be a homebody who would rather go to dinner and a movie than the lake or anywhere outdoors. It’s not that my husband doesn’t enjoy the outdoors — he does. It’s that I have never had the self-assurance to actually enjoy the outdoors. Anyone whose thighs rub together can tell you how miserable being outside in the summer can be.
Beyond that, I’ve never felt comfortable using outdoor furniture. I would avoid picnics and barbecues because the white or green plastic patio furniture most people have wouldn’t fit me or, even worse, would break under my weight.
Being the life of the party is one thing, but being the person who gets laughed at because she broke a chair and fell to the ground is entirely different.
I know from experience.
So as I got bigger, my world became smaller. Now the reverse is occurring.
I’m losing weight at what feels like a rapid pace, and the world is opening up to me just as quickly. My husband and I are making plans for activities and getaways that I only dreamed about before. We’re talking about flying to New England in the fall to visit friends and see the leaves change color. That’s possible, because I won’t have to worry about fitting in an airplane seat anymore. And I hope to spend some time on a friend’s houseboat this summer. I’m even going swimsuit shopping this weekend to prove my willingness.
I know we’re going to be a much more social couple this year than ever before, and the prospect is equally scary and exciting. Doors are wide open for us, as if there’s a whole new life waiting for us out there.
It’s as if I have a chance to be a child again.Now that I don’t have to be as concerned about social catastrophes related to my size, I’m more willing to attend those backyard barbecues, picnics and houseboat parties. And who knows what that will lead to? For the first time in my life, I’m open to new adventures.
Before having gastric-bypass surgery, I loathed placing myself in the category of being overweight. I considered myself more active and more nutritionally educated than most of my peers, obese or not. I also thought I had more confidence than other women. I had a husband who never complained and thought I was gorgeous. I paid attention to my appearance and tried my best not to be slovenly.
Of course, the bigger I got, the less those things seemed important or even possible and the more I saw myself as a hopelessly obese person. I felt that there was no point trying to improve myself because it wasn’t possible or even worth the trouble.
Taking the elevator to my second-floor office became more of a necessity than an example of laziness. My knees just couldn’t handle lugging all 300-plus pounds of me up a single flight of stairs. Even getting out of my office chair to walk across the room to the printer seemed an impossible feat.
At home, things were no better. I stopped painting my toenails because I couldn’t reach my feet. Shaving my legs stopped being an absentminded shower habit and started requiring advanced planning. When would I have time to lock myself in the bathroom for hours as I tried to contort myself to reach hairy patches of skin with a sharp blade? To be truthful, I lost the energy to even think about shaving.
While others spent their weekends planning hiking, skiing or boating trips, I preferred to be a homebody who would rather go to dinner and a movie than the lake or anywhere outdoors. It’s not that my husband doesn’t enjoy the outdoors — he does. It’s that I have never had the self-assurance to actually enjoy the outdoors. Anyone whose thighs rub together can tell you how miserable being outside in the summer can be.
Beyond that, I’ve never felt comfortable using outdoor furniture. I would avoid picnics and barbecues because the white or green plastic patio furniture most people have wouldn’t fit me or, even worse, would break under my weight.
Being the life of the party is one thing, but being the person who gets laughed at because she broke a chair and fell to the ground is entirely different.
I know from experience.
So as I got bigger, my world became smaller. Now the reverse is occurring.
I’m losing weight at what feels like a rapid pace, and the world is opening up to me just as quickly. My husband and I are making plans for activities and getaways that I only dreamed about before. We’re talking about flying to New England in the fall to visit friends and see the leaves change color. That’s possible, because I won’t have to worry about fitting in an airplane seat anymore. And I hope to spend some time on a friend’s houseboat this summer. I’m even going swimsuit shopping this weekend to prove my willingness.
I know we’re going to be a much more social couple this year than ever before, and the prospect is equally scary and exciting. Doors are wide open for us, as if there’s a whole new life waiting for us out there.
It’s as if I have a chance to be a child again.Now that I don’t have to be as concerned about social catastrophes related to my size, I’m more willing to attend those backyard barbecues, picnics and houseboat parties. And who knows what that will lead to? For the first time in my life, I’m open to new adventures.
Saturday, June 04, 2005
The side effects of weight loss
Originally published June 4, 2005, in Our Town for the Tracy Press.
I’m constantly amazed at the differences between the person I was before surgery and the person I’m becoming. I say “becoming,” because I’m changing in various ways all the time.
I’m not the first person in the world to lose weight — nor am I the only person who has ever undergone weight-loss surgery — so most of the changes aren’t unique to me. And yet, for me, they are unique. In fact, they’re shocking.
Every woman's dreamEvery women’s magazine features stories that tell of better body image, increased self confidence, new-found energy and a general improvement in quality of life after weight loss. But few of us get to experience those feelings for ourselves because, as the media frequently points out, dieting has a 95 percent failure rate.Having spent much of my life among the 95 percent, I would read those articles and dream that I would one day have similar success. I could probably recite the basic formula for those published success stories on demand.
Giving upI was a loyal subscriber of both Shape and Self magazines from the time I was 17 years old until late last year. I spent so many years reading the magazines because they provided what I considered to be balanced information regarding diet and exercise, and I was hooked on the readers’ success stories featured in every issue.
I stopped subscribing because I realized those magazines negatively affected my self-esteem. Every issue featured a new eating plan that I didn’t have the money or time to start or stick to and a workout plan that I didn’t have the physical ability to follow.Every month, I’d feel like more and more of a failure, until I eventually stopped reading them all together.
A new perspectiveI hadn’t so much as glanced at a fitness magazine until last weekend, when I picked up a copy of Shape at the newsstand. I grabbed it because it had a workout plan that I thought could help me add a little variety to my exercise routine.
Flipping through the pages, I found myself easily sucked in to the success stories, as always. The difference now was that I didn’t look at those stories to be a measure of my failure.
As I looked over the workout plans featured, I saw quite a few exercises that I would be comfortable incorporating into my routine. The most useful feature I saw was “Remodel Your Butt,” which professes, “Big butt, no butt, droopy butt? Reshape your assets just in time for swimsuit season with our six super-effective moves.”
I know it won’t get me to my “best bikini bod” in 30 days, as the magazine promises. But the exercises shown are an appealing addition to my workout routine.
Aside from my new outlook regarding fitness magazines, I have an ever-changing outlook on myself.
A month ago, I was jumping up and down because I could reach my feet to paint my toenails. Last week, I indulged in a pedicure, because I finally wasn’t afraid of being “too big” for the pedicure chairs. Of course, the fact that my feet don’t swell up like potatoes anymore makes me a little more interested in their appearance.Speaking of appearances, I’m rarely willing to leave the house anymore without at least a little makeup and some attempt at styling my hair (what little I have).
In the months before surgery, when I felt like I was choking on my own fat, I would have said that I just wasn’t vain enough to worry about trivial things like makeup and hairstyles.But the truth is that I don’t think vanity — in healthy doses — is a bad thing. And though I wish I could have felt this good about myself before gastric-bypass surgery, I’m thankful I’m experiencing it now.
I’m constantly amazed at the differences between the person I was before surgery and the person I’m becoming. I say “becoming,” because I’m changing in various ways all the time.
I’m not the first person in the world to lose weight — nor am I the only person who has ever undergone weight-loss surgery — so most of the changes aren’t unique to me. And yet, for me, they are unique. In fact, they’re shocking.
Every woman's dreamEvery women’s magazine features stories that tell of better body image, increased self confidence, new-found energy and a general improvement in quality of life after weight loss. But few of us get to experience those feelings for ourselves because, as the media frequently points out, dieting has a 95 percent failure rate.Having spent much of my life among the 95 percent, I would read those articles and dream that I would one day have similar success. I could probably recite the basic formula for those published success stories on demand.
Giving upI was a loyal subscriber of both Shape and Self magazines from the time I was 17 years old until late last year. I spent so many years reading the magazines because they provided what I considered to be balanced information regarding diet and exercise, and I was hooked on the readers’ success stories featured in every issue.
I stopped subscribing because I realized those magazines negatively affected my self-esteem. Every issue featured a new eating plan that I didn’t have the money or time to start or stick to and a workout plan that I didn’t have the physical ability to follow.Every month, I’d feel like more and more of a failure, until I eventually stopped reading them all together.
A new perspectiveI hadn’t so much as glanced at a fitness magazine until last weekend, when I picked up a copy of Shape at the newsstand. I grabbed it because it had a workout plan that I thought could help me add a little variety to my exercise routine.
Flipping through the pages, I found myself easily sucked in to the success stories, as always. The difference now was that I didn’t look at those stories to be a measure of my failure.
As I looked over the workout plans featured, I saw quite a few exercises that I would be comfortable incorporating into my routine. The most useful feature I saw was “Remodel Your Butt,” which professes, “Big butt, no butt, droopy butt? Reshape your assets just in time for swimsuit season with our six super-effective moves.”
I know it won’t get me to my “best bikini bod” in 30 days, as the magazine promises. But the exercises shown are an appealing addition to my workout routine.
Aside from my new outlook regarding fitness magazines, I have an ever-changing outlook on myself.
A month ago, I was jumping up and down because I could reach my feet to paint my toenails. Last week, I indulged in a pedicure, because I finally wasn’t afraid of being “too big” for the pedicure chairs. Of course, the fact that my feet don’t swell up like potatoes anymore makes me a little more interested in their appearance.Speaking of appearances, I’m rarely willing to leave the house anymore without at least a little makeup and some attempt at styling my hair (what little I have).
In the months before surgery, when I felt like I was choking on my own fat, I would have said that I just wasn’t vain enough to worry about trivial things like makeup and hairstyles.But the truth is that I don’t think vanity — in healthy doses — is a bad thing. And though I wish I could have felt this good about myself before gastric-bypass surgery, I’m thankful I’m experiencing it now.
Friday, March 25, 2005
Different worlds: Life before, during and after gastric-bypass surgery




Originally published March 28, 2007, in the Tracy Press.
A couple of years ago, my husband and I stopped at a diner on Highway 132 for breakfast on the
way to Turlock. We were seated at a dinky table because I had outgrown the diner’s booths years before. Two tables over was a middle-aged couple. While I was perusing the menu, I couldn’t help but notice that the couple seemed to be talking about us. I ignored it, thinking it was just my insecurity.
My husband and I ordered our beverages and breakfast, and he excused himself for a moment.
He had been gone about five minutes when the man from the other table got up and approached me. He introduced himself and told me he had once been like me.
He had been gone about five minutes when the man from the other table got up and approached me. He introduced himself and told me he had once been like me.
Unsure of what he meant, I smiled and let him continue.
He told me he had recently undergone gastric-bypass
surgery and that it had changed his life. He encouraged
me to do the same. He said he had wasted too many
years of his life in an obese prison and that he couldn’t
bear to see someone as young as me do the same.
Shock treatment
Floored, I managed to stammer out some pleasant-sounding questions. Inside, I wasn’t sure if I should burst into tears or punch out his teeth. He told me he had been disabled and unable to walk or drive before the procedure.
He talked about having a new lease on life and feeling that God compelled him to talk to others he saw struggling with their weight. Not sure how to respond to such passion, I quietly thanked him for his time and cursed my husband for leaving the table. I was sure the man wouldn’t have had the nerve to approach me had he been there. But even if he had, my husband surely would have punched his teeth out.
The man and his wife left soon after our talk, and my husband came back to the table just as our food arrived. As I picked over my food, my emotions ran the gamut from anger to shock to despair to shock and back to anger. I tried to numb the emotions by eating the oversize platter of eggs, sausage and hash browns I was served. It didn’t work; instead, my stomach just started to hurt.
Finally, I told my husband. Though he took my side and said the man was either delusional or
just so happy with his own results that he couldn’t help his eagerness to share it with the world, the man’s words stuck.
just so happy with his own results that he couldn’t help his eagerness to share it with the world, the man’s words stuck.
It wasn’t something I ever said out loud, but I was miserable. The truth was that I was bloated and swollen and feeling like a stranger in my own body. But I didn’t know how to admit it.
Reality sinks in
About a year ago, as I sat on a cold exam table in a paper nightgown, my doctor told me I had obesity-related infertility.
About a year ago, as I sat on a cold exam table in a paper nightgown, my doctor told me I had obesity-related infertility.
I was crushed.
I fell into a depression. Not the kind of depression that’s diagnosed by doctors and medicated, but the kind that makes you hate everyone and everything and become a general pain to be around. My weight quickly jumped from 280 pounds up to 335, and I would bet I went as high as 345.
Finally, I began to consider surgical weight loss. It was one thing when the only miserable person was me, but now my husband was sad because we couldn’t have that family we wanted so badly.
Feb. 23
Tonight, the day before I have gastric-bypass surgery, it’s the man in the diner who is on my mind. I’ve been pretty stoic today, but my mind has gone a million miles a minute with the idea of going through with this.
Tonight, the day before I have gastric-bypass surgery, it’s the man in the diner who is on my mind. I’ve been pretty stoic today, but my mind has gone a million miles a minute with the idea of going through with this.
Everybody has a different way of coping with stress. I spend some time with family and friends, but I really crave time alone. I manage tonight to get about an hour of it. My husband, on the other hand, prefers a six pack of Corona to the company of friends or to being alone.
Once he returns to the room, the floodgates open. As we cuddle in bed, I begin to cry uncontrollably. As is typical for my man-of-few-words husband, he just holds me and hands me tissues at the appropriate times. Once my sobs quiet, he asks if I am OK.
I tell him I’m worried that I won’t be able to adjust to the lifestyle that this surgery
requires. I’m sure he thinks the comment was ridiculous. After all, I can tell from the look he’s worn all day that he is more worried about becoming a widower than anything else.
requires. I’m sure he thinks the comment was ridiculous. After all, I can tell from the look he’s worn all day that he is more worried about becoming a widower than anything else.
But he doesn’t mock me.
Instead, he responds with the type of comment that reminds me why I married him in the first place.
“You can do anything you set your mind to; this will be hard, but you’ve handled much more difficult challenges before. You’ll do great.”
And with that, we both fall asleep.
Feb. 24
It’s about 7:30 a.m., time to say goodbye to my family. Ihug my best friend, my husband, my mom and my mother- in-law, all of whom caravanned from the valley to South San Francisco.
It’s about 7:30 a.m., time to say goodbye to my family. Ihug my best friend, my husband, my mom and my mother- in-law, all of whom caravanned from the valley to South San Francisco.
I’m taken back into a large room with gurneys lined in rows that have curtains separating them.
Behind curtains, I’m told to remove all my clothing and put on thin socks, an extra-large hospital gown and a blue paper shower cap. I put all my belongings into a plastic bag that will be given to my husband when I’m sent in for surgery. They let me keep on my glasses until the last minute.
Behind curtains, I’m told to remove all my clothing and put on thin socks, an extra-large hospital gown and a blue paper shower cap. I put all my belongings into a plastic bag that will be given to my husband when I’m sent in for surgery. They let me keep on my glasses until the last minute.
I’m surprised at how cold the operating room is. I guess that’s one way to control a patient’s bleeding — operate in sub-zero temperatures. Once on the operating table, a pillow is put behind my head. My last memory is that of reaching back to adjust it.
Post-op
I wake up in ICU two hours later in terrible pain. I tell the nurse it feels as if I’ve been kicked by a cow. She doesn’t realize I’m speaking from experience.
I wake up in ICU two hours later in terrible pain. I tell the nurse it feels as if I’ve been kicked by a cow. She doesn’t realize I’m speaking from experience.
I’m asked my pain level, and I rate it a four out of 10. Actually, it’s an eight. I just can’t think clearly enough to make sense of the question at the moment.
The nurse asks if I want visitors, and I bark at her.
“I don’t want anybody to see me like this.”
She turns the lights on; I make her turn them off. She hands me a control to the morphine drip. She tells me that I’m already getting morphine in my IV, but that I can hit the button every 10 minutes for an extra gram. I squint at the clock because I don’t have my glasses. Fifteen minutes later, I open my eyes and press the button.
The nurse tries to point out everything in the room, but I tell her I can’t see without my glasses.
She asks if she can get my husband to bring them to me. I want to say no because I don’t want him to see me in pain, but I’m overcome by the need to see. I hit the button
again. It’s about 11 a.m.
She asks if she can get my husband to bring them to me. I want to say no because I don’t want him to see me in pain, but I’m overcome by the need to see. I hit the button
again. It’s about 11 a.m.
Find my husband
I manage to give the nurse a detailed description of my husband, “He’s really tall and really
blond, and please don’t call him Mr. Luiz. He hates that; we have different last names.”
I manage to give the nurse a detailed description of my husband, “He’s really tall and really
blond, and please don’t call him Mr. Luiz. He hates that; we have different last names.”
A few minutes later, I hear her talking to him.
“She’s doing great. She’s in a lot of pain, but she was alert enough to describe you to a tee.”
My husband walks in, kisses me and gives me my glasses. He looks like he hasn’t slept in days. I ask him if he’s been pacing.
“I think I took the floor down five inches,” he answers.
I tell him he looks worried; he says he feels better now. I tell him that I feel like I’ve been kicked by a cow. He laughs. He’s been kicked by a cow before, too.
The nurse asks if I’m ready for more visitors. The answer is still no. My husband leans close and says that my best friend and mom want to come in. My best friend, who drove from Modesto, won’t leave until she sees me. I agree to let her and my mom in because I don’t wantmy friend to hit traffic. I tell my husband to send them in.
“But tell them they can’t stay very long,” I call after him.
Anodyne and love
Right before my mom and best friend enter my room, I press the morphine button again. I don’t even look at the clock this time. I let them both hug me, and I tell them I’m fine, just in a little pain. My mom tries to rub my feet. I beg her not to touch me. I tell them I want to sleep and that I want to see my husband again. They leave, but more people are waiting to see me.
Right before my mom and best friend enter my room, I press the morphine button again. I don’t even look at the clock this time. I let them both hug me, and I tell them I’m fine, just in a little pain. My mom tries to rub my feet. I beg her not to touch me. I tell them I want to sleep and that I want to see my husband again. They leave, but more people are waiting to see me.
When Beau returns, I tell him how much I love him. I’m so tired. I tell him I really want to go to sleep. His mom still wants to come in, but she promises not to stay long. He tells me that I
can sleep after that, and he and my family will go to lunch. After my mother-in-law comes in and gives me a hug and a kiss, I fall asleep.
can sleep after that, and he and my family will go to lunch. After my mother-in-law comes in and gives me a hug and a kiss, I fall asleep.
The sleep isn’t incredibly restful. I’m intermittently interrupted by visits from the anesthesiologist, surgeon, health educator and other medical professionals I don’t remember. But when I wake up at 1:30 p.m., I feel like a new woman.
Four weeks later
I don’t feel like I’ve had major surgery. In fact, when I’m not eating, it’s easy to forget that anything has been done to my digestive system. But something has, and I’d be lying if I said it hasn’t been a major adjustment.
I don’t feel like I’ve had major surgery. In fact, when I’m not eating, it’s easy to forget that anything has been done to my digestive system. But something has, and I’d be lying if I said it hasn’t been a major adjustment.
Spontaneity is no longer in my vocabulary. Every time I plan to leave the house, I have to have an itinerary. I need to know how long I’ll be gone, where I’m going and how that will affect
mealtime. Most times, I pack an ice chest before I leave. Regardless of where the day takes me, it ensures I won’t have to worry about cutting my day short to forage for food. It also adds a good half hour of preparation to my day.
mealtime. Most times, I pack an ice chest before I leave. Regardless of where the day takes me, it ensures I won’t have to worry about cutting my day short to forage for food. It also adds a good half hour of preparation to my day.
I have to make sure the ice chest has foods I can eat that add up to 80 grams of protein — my daily requirement — in case I’m out past dinner. Of course, most of the food has to be ready to eat because I never know whether I’ll be somewhere with a microwave at my disposal.
A clockwork diet
Once the food situation is figured out, then I have to organize a travel pill box with my vitamins. I have to take a multivitamin twice a day, iron once a day and calcium six times a day. None of the vitamins can be taken with the others, and they also must be taken no fewer than two hours apart.
Once the food situation is figured out, then I have to organize a travel pill box with my vitamins. I have to take a multivitamin twice a day, iron once a day and calcium six times a day. None of the vitamins can be taken with the others, and they also must be taken no fewer than two hours apart.
Then, there is the water. Drinking 64 ounces of water isn’t easy anywhere — especially when the size of my mouth is more than double the size of my new pouch — but it’s even more difficult when traveling. I keep a stash of liter-size water bottles for traveling. I also keep extra bottles in the car, just in case I’m stranded somewhere.
After I’ve done all that, I check the clock. Let’s say it’s 10 a.m. Generally, I finish my breakfast at 8:30 a.m. That means I have to have lunch at 1:30 p.m. and dinner at 7 p.m. If, for some reason, I miss my mealtime by 30 minutes or an hour, my whole day will be thrown off.
I also have to plot my water consumption around my meals because I have to abstain from fluids for 10 minutes before a meal and for an hour afterward. That means I have 3½waking hours when I’m not allowed to consume fluids.
Aside from day-to-day logistics regarding meals, vitamins and water, I have to be diligent about getting my exercise. I have to admit, this and water consumption are my weakest areas. I’m still easily exhausted. I am not consuming more than 500 calories a day, and I’m trying to balance work and a personal life on that minimal amount of fuel.
Me first, by necessity
When I overdo it and get exhausted, exercise suffers. At the moment, I need 10 hours of sleep just to function. Before surgery, I easily operated on four . If I don’t get 10 hours now, it’s very hard to get out of bed in the morning for work, much less to go tothe gym. However, that’s no excuse.
When I overdo it and get exhausted, exercise suffers. At the moment, I need 10 hours of sleep just to function. Before surgery, I easily operated on four . If I don’t get 10 hours now, it’s very hard to get out of bed in the morning for work, much less to go tothe gym. However, that’s no excuse.
My husband reminds me that
gastric bypass forces a person to put him or herself first. And that getting enough exercise is one of the main ways I can focus on myself. I’m lucky to have him for a reality check.
gastric bypass forces a person to put him or herself first. And that getting enough exercise is one of the main ways I can focus on myself. I’m lucky to have him for a reality check.
In the past four weeks, I have lost 30 pounds. Not too bad, if I say so myself. But, I’d be lying if I said I’m not still self-critical. I know a few people who weighed the same amount as me before surgery, and they dropped 50 pounds the first month. It’s hard not to compare
myself to them. But part of the reason I had this surgery is that I’m not typical.
myself to them. But part of the reason I had this surgery is that I’m not typical.
My body has never responded well to weight-loss programs, so I don’t know why it surprises me that it would be slower than most to lose weight after bypass surgery. If anything, I can say every day is a lesson for me. I’m more in tune with my body than ever before. And though the adjustment hasn’t happened overnight, the fact that it has happened at all amazes me.
Saturday, January 29, 2005
The Devil is in the details
Originally published Jan. 29, 2005, in the Tracy Press
A little over a month ago, I began writing this column with the idea that I would have gastric- bypass surgery sometime between March and August of this year.
It’s amazing to me how so much can change in what feels like the blink of an eye. It turns out that in just four short weeks from now, I will go under the knife to have my digestive system rerouted to facilitate rapid weight loss — to the tune of about 100 pounds in the first year — in the hopes of overcoming obesity-related infertility.
It’s almost surreal as I think back to how this occurred.
A few weeks ago, I was crying in my soup about how the holidays were a little too festive for me. I talked about how I needed to get back on track because I was meeting with the hospital bariatric team’s medical director, and I wanted to make a good impression by not gaining weight. I succeeded in that. Turns out my scale at home was closer to the hospital scale than I realized, and I weighed in four pounds lighter than in early December. Not too shabby for having a one-week detour around Christmas.
The medical director and I hit it off instantly. We discussed my weight history and the eating habits I learned as a child. She explained her take on my experiences. We talked a bit about my medical history.
And then she said it: “So, Tonya, when would you like to have surgery?”
Stunned, I said, “March?,” thinking she wanted to give me some sort of timeline.
Instead, she said, “You got it.”
I almost couldn’t speak. I managed to stutter, “really?”
Her answer knocked my socks off.
“Well, you’ve lost weight, you’re making life changes, and you don’t have any medical conditions barring you from surgery. You’re a good candidate. Why should we postpone it?”
It’s one thing to believe you’ve earned something, but it’s an entirely different feeling to have the person in control of your reward validate it.
It turns out that March didn’t exactly work out, and I now have a Feb. 24 surgery date. I wasn’t sure whether to jump for joy or burst into tears.
My poor husband wasn’t sure how to take it either. I was so frazzled by the news that I couldn’t even fill out my pre-op forms. He had to do it for me.
Walking out of the office, into the elevator, down four floors and out of the building seemed like a dream.
I don’t think the magnitude of what just happened hit me until the drive home. And then it just exhausted me. I couldn’t stop thinking of everything that needed to be done before surgery.
Some things were little, but everything seemed like a huge boulder of effort.
As soon as we got home, I went straight to the bedroom to lie down. I slept for four hours. The only time I can ever remember sleeping like that was in college the night before I had five difficult finals in the same day. It’s that heavy, drugged sleep your body goes into when your brain is so full of information that you have to be nearly comatose for it to be assimilated.
When I awoke, I was groggy, and everything was still jumbled in my brain. I decided to make myself a late dinner and watch a dumb movie with my husband. I can’t even remember what we watched.
Then, we went to bed. He fell asleep, and I took out my information binder that I was given at my pre-operative orientation in October. I read the entire three-inch binder word for word. Then
I went back to sleep. The next day, I freaked out a little more, repeatedly rattling off everything that had to be done before surgery — balance the checkbook, request time off from work, inform my staff of my upcoming month-long absence and about 50 billion other things I can’t mention here. I must have sounded like Dustin Hoffman in “Rainman,” as I muttered under my breath.
Finally, I took a friend’s advice and made myself a list of everything that needed to be done. Many people have offered to help me, but I’ve yet to take anyone up on it.
After this week, I’ll have three more columns to publish before the day of surgery, and I’ll have to prewrite at least two for part of the time I’m recovering. That gives me five chances to tell readers about my preparations. It doesn’t feel like nearly enough but I’ll give it my best shot.
A little over a month ago, I began writing this column with the idea that I would have gastric- bypass surgery sometime between March and August of this year.
It’s amazing to me how so much can change in what feels like the blink of an eye. It turns out that in just four short weeks from now, I will go under the knife to have my digestive system rerouted to facilitate rapid weight loss — to the tune of about 100 pounds in the first year — in the hopes of overcoming obesity-related infertility.
It’s almost surreal as I think back to how this occurred.
A few weeks ago, I was crying in my soup about how the holidays were a little too festive for me. I talked about how I needed to get back on track because I was meeting with the hospital bariatric team’s medical director, and I wanted to make a good impression by not gaining weight. I succeeded in that. Turns out my scale at home was closer to the hospital scale than I realized, and I weighed in four pounds lighter than in early December. Not too shabby for having a one-week detour around Christmas.
The medical director and I hit it off instantly. We discussed my weight history and the eating habits I learned as a child. She explained her take on my experiences. We talked a bit about my medical history.
And then she said it: “So, Tonya, when would you like to have surgery?”
Stunned, I said, “March?,” thinking she wanted to give me some sort of timeline.
Instead, she said, “You got it.”
I almost couldn’t speak. I managed to stutter, “really?”
Her answer knocked my socks off.
“Well, you’ve lost weight, you’re making life changes, and you don’t have any medical conditions barring you from surgery. You’re a good candidate. Why should we postpone it?”
It’s one thing to believe you’ve earned something, but it’s an entirely different feeling to have the person in control of your reward validate it.
It turns out that March didn’t exactly work out, and I now have a Feb. 24 surgery date. I wasn’t sure whether to jump for joy or burst into tears.
My poor husband wasn’t sure how to take it either. I was so frazzled by the news that I couldn’t even fill out my pre-op forms. He had to do it for me.
Walking out of the office, into the elevator, down four floors and out of the building seemed like a dream.
I don’t think the magnitude of what just happened hit me until the drive home. And then it just exhausted me. I couldn’t stop thinking of everything that needed to be done before surgery.
Some things were little, but everything seemed like a huge boulder of effort.
As soon as we got home, I went straight to the bedroom to lie down. I slept for four hours. The only time I can ever remember sleeping like that was in college the night before I had five difficult finals in the same day. It’s that heavy, drugged sleep your body goes into when your brain is so full of information that you have to be nearly comatose for it to be assimilated.
When I awoke, I was groggy, and everything was still jumbled in my brain. I decided to make myself a late dinner and watch a dumb movie with my husband. I can’t even remember what we watched.
Then, we went to bed. He fell asleep, and I took out my information binder that I was given at my pre-operative orientation in October. I read the entire three-inch binder word for word. Then
I went back to sleep. The next day, I freaked out a little more, repeatedly rattling off everything that had to be done before surgery — balance the checkbook, request time off from work, inform my staff of my upcoming month-long absence and about 50 billion other things I can’t mention here. I must have sounded like Dustin Hoffman in “Rainman,” as I muttered under my breath.
Finally, I took a friend’s advice and made myself a list of everything that needed to be done. Many people have offered to help me, but I’ve yet to take anyone up on it.
After this week, I’ll have three more columns to publish before the day of surgery, and I’ll have to prewrite at least two for part of the time I’m recovering. That gives me five chances to tell readers about my preparations. It doesn’t feel like nearly enough but I’ll give it my best shot.
Saturday, January 22, 2005
What I miss
Originally published Jan. 22, 2005, in the Tracy Press
Last week’s column discussed everything I’m no longer allowed to eat as I prepare to have gastric-bypass surgery. I’ve begun living as if I’ve already had the surgery, which includes abstaining from a host of no-no foods.
When I was considering surgery about a year ago, I realized that I needed to make sure I could live without all my favorites. If I couldn’t live without food that would be verboten, then there was no point in having weight-loss surgery.
I made myself a list of the foods I didn’t think I’d be able to live without forever, and I proceeded to test them. I would prepare the item or order it in a restaurant and reflect on it. I’d take a bite and see if it really tasted as good as I thought it did. I’d see if it felt good on my tongue and whether it felt generally good to eat it.
Surprisingly, most things haven’t been that hard to give up. But I think others will be a challenge for the rest of my life. I’m willing to take the challenge because I believe the benefits of surgery are worth it.
Here’s a rundown of what I found:
What I don’t miss
• Soda — I hadn’t really liked soda as a child, so giving it up was easy.
• Carbonation — As much as I love mineral water, I don’t miss it.
• Gum — I still think Dentyne Ice is the best remedy for after-lunch breath, but sugar-free breath mints will suffice.
• Coconut — The only time I eat coconut is when it’s in candy or desserts, and those are already forbidden (more on that later).
• Beef jerky — Since I don’t eat beef, it’s a non-issue.
What I do miss
• Alcohol — Drinking water at a party seems to make more of a spectacle of me than the drunken girl who dances topless on the bar.
• Fast food — I don’t actually miss the flavor of fast food (except for the grilled-cheese sandwich at In-N-Out), but I do miss the convenience of hitting a drive-through window when I’m short on time.
• Bread — The only reason I miss bread is because it’s very hard to make a sandwich without any.
• Pasta — As if I can imagine going to The Olive Garden and ordering anything else. I really don’t like minestrone soup, so this may be a restaurant I don’t eat at after surgery.
• Rice — Tofu curry from the Thai Café on Central Avenue just doesn’t taste good when it’s not combined with jasmine rice.
• Spicy food — Mild salsa just doesn’t enhance Mexican food as well as the hotter varieties.
• Desserts — This is almost deserving of its own column. I love desserts. Anything sweet and creamy has my vote. Cover it in chocolate and I consider it unbeatable.
I have to be honest: That list I made about a year ago specifying all the foods I wanted to see if I could live without consisted almost entirely of desserts. Sure, the In-N-Out grilled cheese was on the list, but it only took one bite for me to realize that I could live the rest of my life without eating another one. The chocolate mousse cake from Fabio’s, on the other hand, took three tries before I could resign myself to the idea of living without it (Yes, it really is that good).
I couldn’t begin to discuss my love for rich desserts, particularly when paired with a glass of vintage port wine. No dessert has ever been too rich for me — not even the decadent chocolate truffle pie at Magellan’s.
Even fast food — which I subsisted on for at least five days a week — wasn’t as hard to give up.
The deciding factor for me going through with gastric-bypass surgery is the realization that food is fleeting.
Yes, I love Marie Callender’s pies and the blended Carmelo Sensation at Zizzo’s on 10th Street. But I love the idea of fitting into the seats on amusement park rides so much more. The idea of climbing up the rock formations at Mount Diablo with my husband is as intoxicating as any ice cream creation at Cold Stone Creamery.
And the best feeling I can imagine is becoming pregnant and giving birth to my own child. And I know that won’t happen for me without surgery.
When it comes to the idea of having a baby, the richest dessert in the world holds no comparison.
Last week’s column discussed everything I’m no longer allowed to eat as I prepare to have gastric-bypass surgery. I’ve begun living as if I’ve already had the surgery, which includes abstaining from a host of no-no foods.
When I was considering surgery about a year ago, I realized that I needed to make sure I could live without all my favorites. If I couldn’t live without food that would be verboten, then there was no point in having weight-loss surgery.
I made myself a list of the foods I didn’t think I’d be able to live without forever, and I proceeded to test them. I would prepare the item or order it in a restaurant and reflect on it. I’d take a bite and see if it really tasted as good as I thought it did. I’d see if it felt good on my tongue and whether it felt generally good to eat it.
Surprisingly, most things haven’t been that hard to give up. But I think others will be a challenge for the rest of my life. I’m willing to take the challenge because I believe the benefits of surgery are worth it.
Here’s a rundown of what I found:
What I don’t miss
• Soda — I hadn’t really liked soda as a child, so giving it up was easy.
• Carbonation — As much as I love mineral water, I don’t miss it.
• Gum — I still think Dentyne Ice is the best remedy for after-lunch breath, but sugar-free breath mints will suffice.
• Coconut — The only time I eat coconut is when it’s in candy or desserts, and those are already forbidden (more on that later).
• Beef jerky — Since I don’t eat beef, it’s a non-issue.
What I do miss
• Alcohol — Drinking water at a party seems to make more of a spectacle of me than the drunken girl who dances topless on the bar.
• Fast food — I don’t actually miss the flavor of fast food (except for the grilled-cheese sandwich at In-N-Out), but I do miss the convenience of hitting a drive-through window when I’m short on time.
• Bread — The only reason I miss bread is because it’s very hard to make a sandwich without any.
• Pasta — As if I can imagine going to The Olive Garden and ordering anything else. I really don’t like minestrone soup, so this may be a restaurant I don’t eat at after surgery.
• Rice — Tofu curry from the Thai Café on Central Avenue just doesn’t taste good when it’s not combined with jasmine rice.
• Spicy food — Mild salsa just doesn’t enhance Mexican food as well as the hotter varieties.
• Desserts — This is almost deserving of its own column. I love desserts. Anything sweet and creamy has my vote. Cover it in chocolate and I consider it unbeatable.
I have to be honest: That list I made about a year ago specifying all the foods I wanted to see if I could live without consisted almost entirely of desserts. Sure, the In-N-Out grilled cheese was on the list, but it only took one bite for me to realize that I could live the rest of my life without eating another one. The chocolate mousse cake from Fabio’s, on the other hand, took three tries before I could resign myself to the idea of living without it (Yes, it really is that good).
I couldn’t begin to discuss my love for rich desserts, particularly when paired with a glass of vintage port wine. No dessert has ever been too rich for me — not even the decadent chocolate truffle pie at Magellan’s.
Even fast food — which I subsisted on for at least five days a week — wasn’t as hard to give up.
The deciding factor for me going through with gastric-bypass surgery is the realization that food is fleeting.
Yes, I love Marie Callender’s pies and the blended Carmelo Sensation at Zizzo’s on 10th Street. But I love the idea of fitting into the seats on amusement park rides so much more. The idea of climbing up the rock formations at Mount Diablo with my husband is as intoxicating as any ice cream creation at Cold Stone Creamery.
And the best feeling I can imagine is becoming pregnant and giving birth to my own child. And I know that won’t happen for me without surgery.
When it comes to the idea of having a baby, the richest dessert in the world holds no comparison.
Saturday, January 15, 2005
What not to eat
Originally published Jan. 15, 2005.
I mentioned last week that I have to start living my life as if I have already had gastric-bypass surgery. This means, I must exercise regularly and eat differently.
Exercising regularly is a no-brainer. I’m expected to exercise at least 30 minutes a day, six days a week. This will help get my body in shape to recover faster from surgery. Exercising regularly now also means that I’ll be more able to increase my workouts after surgery. Most patients I’ve spoken to exercise one to two hours a day, six days a week.
Having spent much of my life trying to control my weight, I’m familiar with exercise.
I like doing yoga and lifting weights. Pilates is fun, but I have trouble completing an hour-long session. Cardio is my least favorite form of exercise, but I have grown to enjoy using an elliptical cross-trainer at the gym. The zero-impact motion is easy on my knees without being too easy on the rest of me.
I’ve been told cardiovascular exercise will help my body better handle the effects of anesthesia, though I have yet to confirm this with a surgeon; however, doctors have told me that strength training now will help me to preserve my muscle mass during recovery. Building my stomach muscles should also help my abdominal wall heal from the incision wounds faster.
Aside from needing to be better about scheduling my workout as if it were any other unbreakable appointment, I’ve gotten the exercise component down pat.
The more difficult aspect of preparing for surgery is eating differently. I’ve grown accustomed to my new eating habits and am comfortable with them now, but that wasn’t the case three months ago when I received my pre-operative eating requirements.
Except for the week of Christmas, I’ve diligently followed my prescribed 1,200- calorie-a-day eating plan for the past 12 weeks. As I touched on last week, though, there is a lot more to my new plan than just watching calories.
Limiting myself to 1,200 calories a day and making sure I consume 80 grams of protein, 133 grams of carbohydrate and no more than 40 grams of fat is easy. But there’s a whole list of rules accompanying that seemingly easy meal plan that is more difficult.
The rules are there to prepare me for life “on the other side.” As such, they don’t make a lot of sense for my body now, but I’m getting ready for when they really do matter.
Here’s a rundown:
• No snacking — I’m supposed to fully fill my pouch at mealtime three times a day. Doing so will enable me to go about five hours between meals with little feeling of hunger.
• No fast foods — Healthy food can be found at fast-food restaurants. But the sights and smells of McDonald’s and Jack In the Box are triggers. For many of us, it’s hard to walk in or go to the drive-through window and only order a salad.
• No caffeine — The stomach pouch has little to no stomach acid. With no acid to dilute it, caffeine could very quickly ulcerate the pouch.
• No carbonated beverages — Carbonation will add gas to the stomach pouch, which can stretch it and enable it to hold more food. Not so good if the idea is to restrict the amount of food consumed in one sitting. Stretching the pouch is also bad because if it’s done too soon after surgery, the staple line could rupture.
• No fluids with meals — This is another rule to help keep the pouch full as long as possible to maintain the feeling of satisfaction. If fluids are consumed with meals, the pouch may empty faster, which means I could eat more in one sitting.
• Avoid starches — Bread gets doughy in the pouch and can clog the outlet, which would be very uncomfortable and could require medical attention to clear.
Because the opening from the pouch to the intestine is only the size of a dime, food must be chewed to the consistency of baby food. Some foods, however, are too difficult to chew that well. These foods include coconut, popcorn, corn and skins and seeds of fruit.
When I first encountered all these rules, I remember thinking that there was no way I could go through with the surgery. There were too many foods I’d have to avoid that I swore I could never live without. But I’ve managed for the last three months, and I don’t miss many of the things I thought I would.
How did I accomplish this? That’s what next week’s column is about.
I mentioned last week that I have to start living my life as if I have already had gastric-bypass surgery. This means, I must exercise regularly and eat differently.
Exercising regularly is a no-brainer. I’m expected to exercise at least 30 minutes a day, six days a week. This will help get my body in shape to recover faster from surgery. Exercising regularly now also means that I’ll be more able to increase my workouts after surgery. Most patients I’ve spoken to exercise one to two hours a day, six days a week.
Having spent much of my life trying to control my weight, I’m familiar with exercise.
I like doing yoga and lifting weights. Pilates is fun, but I have trouble completing an hour-long session. Cardio is my least favorite form of exercise, but I have grown to enjoy using an elliptical cross-trainer at the gym. The zero-impact motion is easy on my knees without being too easy on the rest of me.
I’ve been told cardiovascular exercise will help my body better handle the effects of anesthesia, though I have yet to confirm this with a surgeon; however, doctors have told me that strength training now will help me to preserve my muscle mass during recovery. Building my stomach muscles should also help my abdominal wall heal from the incision wounds faster.
Aside from needing to be better about scheduling my workout as if it were any other unbreakable appointment, I’ve gotten the exercise component down pat.
The more difficult aspect of preparing for surgery is eating differently. I’ve grown accustomed to my new eating habits and am comfortable with them now, but that wasn’t the case three months ago when I received my pre-operative eating requirements.
Except for the week of Christmas, I’ve diligently followed my prescribed 1,200- calorie-a-day eating plan for the past 12 weeks. As I touched on last week, though, there is a lot more to my new plan than just watching calories.
Limiting myself to 1,200 calories a day and making sure I consume 80 grams of protein, 133 grams of carbohydrate and no more than 40 grams of fat is easy. But there’s a whole list of rules accompanying that seemingly easy meal plan that is more difficult.
The rules are there to prepare me for life “on the other side.” As such, they don’t make a lot of sense for my body now, but I’m getting ready for when they really do matter.
Here’s a rundown:
• No snacking — I’m supposed to fully fill my pouch at mealtime three times a day. Doing so will enable me to go about five hours between meals with little feeling of hunger.
• No fast foods — Healthy food can be found at fast-food restaurants. But the sights and smells of McDonald’s and Jack In the Box are triggers. For many of us, it’s hard to walk in or go to the drive-through window and only order a salad.
• No caffeine — The stomach pouch has little to no stomach acid. With no acid to dilute it, caffeine could very quickly ulcerate the pouch.
• No carbonated beverages — Carbonation will add gas to the stomach pouch, which can stretch it and enable it to hold more food. Not so good if the idea is to restrict the amount of food consumed in one sitting. Stretching the pouch is also bad because if it’s done too soon after surgery, the staple line could rupture.
• No fluids with meals — This is another rule to help keep the pouch full as long as possible to maintain the feeling of satisfaction. If fluids are consumed with meals, the pouch may empty faster, which means I could eat more in one sitting.
• Avoid starches — Bread gets doughy in the pouch and can clog the outlet, which would be very uncomfortable and could require medical attention to clear.
Because the opening from the pouch to the intestine is only the size of a dime, food must be chewed to the consistency of baby food. Some foods, however, are too difficult to chew that well. These foods include coconut, popcorn, corn and skins and seeds of fruit.
When I first encountered all these rules, I remember thinking that there was no way I could go through with the surgery. There were too many foods I’d have to avoid that I swore I could never live without. But I’ve managed for the last three months, and I don’t miss many of the things I thought I would.
How did I accomplish this? That’s what next week’s column is about.
Saturday, January 08, 2005
Getting back on track
Originally published Jan. 8, 2005, in the Tracy Press.
As the first week of the new year comes to a close, I have to say I spent it like most people — making up for the sins of the holidays.
What many refer to as a New Year’s resolution is a means to an end for me. I need to lose about 30 pounds to be cleared for gastric-bypass surgery through my insurer. I was given that weight goal at my pre-operative orientation in mid- October. Between that day and my visit with the program’s dietician in early December, I had lost nine pounds. The dietician seemed impressed, especially considering that I met with her the week after Thanksgiving.
Unfortunately, the week of Christmas brought a setback. It’s never the day of the holiday that gets me. With plenty of people to visit with, I find myself too distracted to overeat. What seems to be my downfall is the time preceding a holiday, when I’m too scatterbrained to pay attention to what I’m putting in my mouth. And I tend to lose my resolve at work.
Holidays are a tough time in most offices — everyone is doing extra work to make up for the shorter workweeks or to fill in for those on vacation, not to mention dealing with the seemingly endless supply of treats dropped off by clients or brought in by co-workers.
After giving in to a truffle, it became easier to say yes to fudge, cookies and gourmet coffee drinks. And the easier it was to say yes, the harder it was to say no. And that’s why I spent Christmas night realizing that the jeans that had been so loose the week before now protested every time I tried to lift the zipper.
I spent much of last week thinking about how I was going to get back on track. It felt like I had all the time in the world — until I pulled out my 2005 calendar and realized I had a little more than a week before my next weigh-in.
As you read this column, I will be on my way to San Francisco to meet with the bariatric program director at the hospital where I’m expected to have surgery.
The director has the power to schedule my surgery for two weeks — or even two years — from when we meet. Showing up with a 10-pound gain is not the way to convey that I’m serious about having surgery.
I’ve had to kick my butt into high gear. I know fad diets don’t work, so I haven’t spent the week fasting or eating nothing but cabbage soup.
I’ve gone back to the preoperative eating plan prescribed by the bariatric team in charge of my case.
Yes, not only do I have to lose weight before surgery, but I’m expected to do it a certain way. The hospital’s way consists of eating 1,200 calories a day in the form of three balanced meals.
Calories aren’t the only thing I have to watch. The bariatric doctors want me to begin living life as if I already have had the surgery. Doing so is meant to prevent me from having transition difficulties after surgery, because not following the dietary rules could kill me.
Within my 1,200 calories a day, I need to consume between 75 and 90 grams of protein, up to 40 grams of fat and no more than 133 grams of carbohydrates.
Though this plan is low in carbs, it’s not a low-carb diet in the traditional sense, because fat and calories are also limited. It’s a low-calorie, low-carb, high-protein and moderate-fat plan.
For the first year after surgery, I will eat anywhere from 500 to 900 calories a day.
Cutting my consumption down to 1,200 now will be a good way to get my body used to reduced nutrients.
The anatomical limitations I’ll have after surgery will prevent me from digesting starchy foods very well, and cutting carbs is better done now than later.
As I’ve explained before, protein will be my main concern after surgery, and it’s best that I focus my energy on lean sources now so I’ll have an easier time later. Not eating red meat or poultry makes it more of challenge, but I’m working on it.
I’m also expected to replace one meal a day with a sugar-free protein supplement that I’m allowed to mix with either milk or water.
Other rules meant to prepare me for surgery include no carbonated beverages, no caffeine and no alcohol.
I’ll tell you a little more about what I can and can’t eat next week. But for now, I need to head to the gym — more on that later, too.
As the first week of the new year comes to a close, I have to say I spent it like most people — making up for the sins of the holidays.
What many refer to as a New Year’s resolution is a means to an end for me. I need to lose about 30 pounds to be cleared for gastric-bypass surgery through my insurer. I was given that weight goal at my pre-operative orientation in mid- October. Between that day and my visit with the program’s dietician in early December, I had lost nine pounds. The dietician seemed impressed, especially considering that I met with her the week after Thanksgiving.
Unfortunately, the week of Christmas brought a setback. It’s never the day of the holiday that gets me. With plenty of people to visit with, I find myself too distracted to overeat. What seems to be my downfall is the time preceding a holiday, when I’m too scatterbrained to pay attention to what I’m putting in my mouth. And I tend to lose my resolve at work.
Holidays are a tough time in most offices — everyone is doing extra work to make up for the shorter workweeks or to fill in for those on vacation, not to mention dealing with the seemingly endless supply of treats dropped off by clients or brought in by co-workers.
After giving in to a truffle, it became easier to say yes to fudge, cookies and gourmet coffee drinks. And the easier it was to say yes, the harder it was to say no. And that’s why I spent Christmas night realizing that the jeans that had been so loose the week before now protested every time I tried to lift the zipper.
I spent much of last week thinking about how I was going to get back on track. It felt like I had all the time in the world — until I pulled out my 2005 calendar and realized I had a little more than a week before my next weigh-in.
As you read this column, I will be on my way to San Francisco to meet with the bariatric program director at the hospital where I’m expected to have surgery.
The director has the power to schedule my surgery for two weeks — or even two years — from when we meet. Showing up with a 10-pound gain is not the way to convey that I’m serious about having surgery.
I’ve had to kick my butt into high gear. I know fad diets don’t work, so I haven’t spent the week fasting or eating nothing but cabbage soup.
I’ve gone back to the preoperative eating plan prescribed by the bariatric team in charge of my case.
Yes, not only do I have to lose weight before surgery, but I’m expected to do it a certain way. The hospital’s way consists of eating 1,200 calories a day in the form of three balanced meals.
Calories aren’t the only thing I have to watch. The bariatric doctors want me to begin living life as if I already have had the surgery. Doing so is meant to prevent me from having transition difficulties after surgery, because not following the dietary rules could kill me.
Within my 1,200 calories a day, I need to consume between 75 and 90 grams of protein, up to 40 grams of fat and no more than 133 grams of carbohydrates.
Though this plan is low in carbs, it’s not a low-carb diet in the traditional sense, because fat and calories are also limited. It’s a low-calorie, low-carb, high-protein and moderate-fat plan.
For the first year after surgery, I will eat anywhere from 500 to 900 calories a day.
Cutting my consumption down to 1,200 now will be a good way to get my body used to reduced nutrients.
The anatomical limitations I’ll have after surgery will prevent me from digesting starchy foods very well, and cutting carbs is better done now than later.
As I’ve explained before, protein will be my main concern after surgery, and it’s best that I focus my energy on lean sources now so I’ll have an easier time later. Not eating red meat or poultry makes it more of challenge, but I’m working on it.
I’m also expected to replace one meal a day with a sugar-free protein supplement that I’m allowed to mix with either milk or water.
Other rules meant to prepare me for surgery include no carbonated beverages, no caffeine and no alcohol.
I’ll tell you a little more about what I can and can’t eat next week. But for now, I need to head to the gym — more on that later, too.
Saturday, January 01, 2005
What makes this time different?
Originally published Jan. 1, 2005, in the Tracy Press.
I ask myself that question all the time. As I mentioned last week, the immediate answer I come up with is: because it has to be.
But that doesn’t really answer the question of what it is about surgical weight loss that makes me think it’ll work when every other diet on the planet has failed.
I hate to sound cliché, but there’s a lot to be said for the journey making all the difference in the world.
I consider myself in a fortunate place right now. I found myself abruptly switching insurance providers last summer just as I was exploring the possibilities of surgical weight loss.
My new insurer is a health maintenance organization with a five-year-old program devoted to weight-loss surgery.
Though weight-loss surgery has been around since the 1970s, few insurers actually have programs in place for members seeking it. It seems more common that insurers require nothing more than a doctor’s referral and leave surgery preparation up to the bariatric specialists with whom they contract.
Every member of my HMO seeking WLS must submit to a process that takes anywhere from 12 to 18 months. The process includes nutrition classes, psychological counseling and lab work — and that’s just to get a patient’s foot in the door.
Once that happens — meaning the HMO’s bariatric program agrees to accept the patient as a surgery candidate — there is still more work to be done.
Everyone must attend a bariatric orientation class at the hospital where he or she will have surgery. The orientation includes a weigh-in and a series of presentations by the hospital’s bariatric team. Patients are told the specifics of gastric-bypass surgery, its pros and cons and the most common complications. A large portion of the day is spent with a nutritionist explaining the vast differences between what patients can eat before surgery vs. after surgery.
The staff also lays down the rules for the program. The most common is a requirement for pre-operative weight loss.
I know it sounds silly, but my insurer expects all bariatric patients to lose 10 percent of their pre-operative weight before they can be cleared for surgery. I’ve heard different justifications for this requirement. Some say that weight-loss shrinks the size of liver, which is very close to the operation site and could be nicked during surgery. Others say it’s necessary because weight loss will reduce belly fat, and the amount of belly fat a person has determines whether surgery can be done laproscopically.
My opinion is that the surgery is expensive, and the HMO doesn’t want to invest its money in patients who aren’t willing to work at being successful. Requiring pre-op weight loss is a way to weed out those who are less than committed. I also believe that the insurer hopes that after losing about 30 pounds — the average patient weighs between 280 and 300 pounds — the patient will change his or her mind about needing surgery.
Some patients remove themselves from the program after orientation either because they don’t feel they can meet all the requirements or because they no longer believe that surgery is the right choice for them. Those who don’t are required to attend further meetings with bariatric nutritionists, psychologists and specialists to make sure they have realistic expectations of surgery and that they are good candidates for surgery. Being a good candidate for surgery, according to my insurer, means the patient is likely to survive the procedure.
As one surgeon told me, “If we’re going to operate, we’d like to be at least 90 percent certain that you’ll wake up when we’re done.”
Apparently, having patients die doesn’t make surgeons very happy.
It’s only after losing 10 percent of their weight and submitting to about a dozen different appointments that patients are truly cleared for surgery and a date is scheduled.
I’m in the midst of this process, and though it can be daunting, I find it comforting.
As someone who has spent thousands of dollars on diet programs, books and pills, I like the fact that I have to work at this. And every obstacle I pass in this process validates that I’m making the right decision.
I attended orientation in October and am now focused on losing about 30 pounds. I did really well in November, dropping nine pounds.
However, the stress of Christmas got the better of me, and I put a bit of that back on.
When I visited the bariatric nutritionist in early December, she told me I was an excellent candidate for fast-tracking, which means I could have the surgery sooner rather than later. She predicted I may have surgery as early as March.
However, I have an appointment Jan. 8 with the program’s medical director. She’s the one who determines whether I get put on that fast track. If I don’t have at least 10 pounds lost by the time I see her, my chances of being fast-tracked are slim.
My focus now is getting back on track. That’s not easy after two weeks of absent-minded indulgence, but it’s a challenge I’m ready to take on.
I ask myself that question all the time. As I mentioned last week, the immediate answer I come up with is: because it has to be.
But that doesn’t really answer the question of what it is about surgical weight loss that makes me think it’ll work when every other diet on the planet has failed.
I hate to sound cliché, but there’s a lot to be said for the journey making all the difference in the world.
I consider myself in a fortunate place right now. I found myself abruptly switching insurance providers last summer just as I was exploring the possibilities of surgical weight loss.
My new insurer is a health maintenance organization with a five-year-old program devoted to weight-loss surgery.
Though weight-loss surgery has been around since the 1970s, few insurers actually have programs in place for members seeking it. It seems more common that insurers require nothing more than a doctor’s referral and leave surgery preparation up to the bariatric specialists with whom they contract.
Every member of my HMO seeking WLS must submit to a process that takes anywhere from 12 to 18 months. The process includes nutrition classes, psychological counseling and lab work — and that’s just to get a patient’s foot in the door.
Once that happens — meaning the HMO’s bariatric program agrees to accept the patient as a surgery candidate — there is still more work to be done.
Everyone must attend a bariatric orientation class at the hospital where he or she will have surgery. The orientation includes a weigh-in and a series of presentations by the hospital’s bariatric team. Patients are told the specifics of gastric-bypass surgery, its pros and cons and the most common complications. A large portion of the day is spent with a nutritionist explaining the vast differences between what patients can eat before surgery vs. after surgery.
The staff also lays down the rules for the program. The most common is a requirement for pre-operative weight loss.
I know it sounds silly, but my insurer expects all bariatric patients to lose 10 percent of their pre-operative weight before they can be cleared for surgery. I’ve heard different justifications for this requirement. Some say that weight-loss shrinks the size of liver, which is very close to the operation site and could be nicked during surgery. Others say it’s necessary because weight loss will reduce belly fat, and the amount of belly fat a person has determines whether surgery can be done laproscopically.
My opinion is that the surgery is expensive, and the HMO doesn’t want to invest its money in patients who aren’t willing to work at being successful. Requiring pre-op weight loss is a way to weed out those who are less than committed. I also believe that the insurer hopes that after losing about 30 pounds — the average patient weighs between 280 and 300 pounds — the patient will change his or her mind about needing surgery.
Some patients remove themselves from the program after orientation either because they don’t feel they can meet all the requirements or because they no longer believe that surgery is the right choice for them. Those who don’t are required to attend further meetings with bariatric nutritionists, psychologists and specialists to make sure they have realistic expectations of surgery and that they are good candidates for surgery. Being a good candidate for surgery, according to my insurer, means the patient is likely to survive the procedure.
As one surgeon told me, “If we’re going to operate, we’d like to be at least 90 percent certain that you’ll wake up when we’re done.”
Apparently, having patients die doesn’t make surgeons very happy.
It’s only after losing 10 percent of their weight and submitting to about a dozen different appointments that patients are truly cleared for surgery and a date is scheduled.
I’m in the midst of this process, and though it can be daunting, I find it comforting.
As someone who has spent thousands of dollars on diet programs, books and pills, I like the fact that I have to work at this. And every obstacle I pass in this process validates that I’m making the right decision.
I attended orientation in October and am now focused on losing about 30 pounds. I did really well in November, dropping nine pounds.
However, the stress of Christmas got the better of me, and I put a bit of that back on.
When I visited the bariatric nutritionist in early December, she told me I was an excellent candidate for fast-tracking, which means I could have the surgery sooner rather than later. She predicted I may have surgery as early as March.
However, I have an appointment Jan. 8 with the program’s medical director. She’s the one who determines whether I get put on that fast track. If I don’t have at least 10 pounds lost by the time I see her, my chances of being fast-tracked are slim.
My focus now is getting back on track. That’s not easy after two weeks of absent-minded indulgence, but it’s a challenge I’m ready to take on.
Saturday, December 25, 2004
The procedure explained
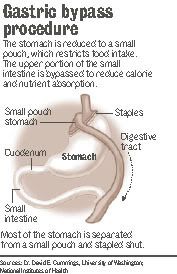
Originally published Dec. 25, 2004, in the Tracy Press.
Touted as the “gold standard” procedure, Roux en Y — often called RNY for short — is considered by my insurer as the only surgical weight-loss method that has proven success. Two celebrities — former talk show host and singer Carnie Wilson and NBC weatherman Al Roker — both used this procedure to lose weight.This procedure will drastically alter the size and capacity of my stomach and reroute my digestive tract.
Weight-loss surgery is a big decision.When I was talking myself into the idea of sharing my story with readers, I told myself that if it prevented one person with unrealistic expectations from having the surgery, it would be a good thing. Now, I realize that I also want to help people who may truly need the surgery but are unaware of how to obtain it.For me, deciding whether to have surgery was difficult, but picking the procedure from the handful available was easy — my insurer only covered one.
Touted as the “gold standard” procedure, Roux en Y — often called RNY for short — is considered by my insurer as the only surgical weight-loss method that has proven success. Two celebrities — former talk show host and singer Carnie Wilson and NBC weatherman Al Roker — both used this procedure to lose weight.This procedure will drastically alter the size and capacity of my stomach and reroute my digestive tract.
My new stomach will be a thumb-sized pouch that connects to about 18 inches of lower intestine. The pouch will stretch to the size of a chicken egg to accommodate food. The procedure is called gastric bypass because much of the gastric system is bypassed.The digestive tract becomes like a sink. Food goes down the drain of the esophagus into the stomach and then empties through another drain into the intestines before it exits the body. The drains are about the size of a dime.
Aside from preventing me from eating much in one sitting and significantly limiting my feelings of hunger, this procedure also will cause unpleasant side effects if I don’t follow the rules. If I don’t chew my food well enough, it will either block the opening between my esophagus and pouch or plug the outlet from my pouch to intestine. Usually, there are two solutions to this problem: vomiting or having a doctor use an endoscope to remove the blockage. Neither sounds like fun to me.
If I eat foods with too much sugar or fat, I may experience dumping syndrome. A phenomenon experienced by about 15 percent of all RNY patients, dumping is described by doctors and former patients as “behavior modification with a vengeance.” The syndrome occurs when a high concentration of sugar or fat is dumped into the intestine. It manifests itself in different ways, but often causes reactions similar to hypoglycemia, such as sweating, feeling faint, heart palpitations and an overwhelming need to lie down. The idea is that after patients experience dumping syndrome once or twice, they stay away from foods loaded with sugar or fat permanently.After surgery, my main dietary focus will be protein.
For the first few weeks with my new digestive system, I will only be able to eat one to two ounces three times a day. That’s not a lot of food. So I will have to work very hard to get in as much protein as possible.
If I don’t get enough protein, I will suffer brittle nails, scaly skin and baldness. I don’t plan to go through this ordeal to end up looking like the Crypt Keeper. Protein also helps maintain muscle mass and the feeling of being satisfied after a meal. I’ll supplement my limited food consumption with a host of vitamins. I’ll take a high-potency multivitamin, calcium and iron every day for the rest of my life. I will also take vitamin B12 under my tongue twice a week because my body will no longer be able to absorb the vitamin through my digestive tract.Vitamin deficiency is linked to permanent hair loss, anemia, hearing loss and other neurological disorders. I’ve already warned my husband that if I start looking AND acting like the Crypt Keeper, crushing up some chewable vitamins in a protein shake should do the trick.
In all seriousness, a lot of work is involved on the part of the patient to ensure the success of gastric bypass.This is not a passive cure-all.As you can see, I will suffer some serious consequences if I don’t follow the post-operative program to the letter.The end-all nature of this is a scary thought for me. I’m the one who has gained and lost the equivalent of two average-sized people in my short time on this planet.What makes me think this time is different? The short answer is: because it has to be. The long answer is fodder for another column, maybe one I’ll write next week.
Saturday, December 18, 2004
A difficult decision made
Originally published Dec. 18, 2004, in the Tracy Press.
I’m officially under the gun to lose weight. I have obesity-related infertility, and if my husband and I hope to conceive the old fashioned way, I need to drop at least 100 pounds. And my doctor suggests I do it sooner rather than later. That’s no easy undertaking.After all, only 5 percent of Americans who diet are successful at maintaining weight loss. I’ve never been among that 5 percent — not even for a minute.
I’ve given up on the commercial weight-loss circuit. It’s not that I don’t believe Weight Watchers, Jenny Craig and similar programs are beneficial. I’ve spent seven years as a WW member, but I’ve never had any long-term success with those types of programs.
I’ve worked with three dieticians in the past two years. They succeeded in helping me improve my food choices and figure out meal planning. One has even helped me make a healthier transition to a pseudo-vegetarian lifestyle (I now abstain from red meat and poultry).But we never succeeded in the realm of weight loss.
I have worked with a couple of therapists on my issues with emotional/binge eating and had great success. It’s been at least six months since I’ve binged, and I no longer use food to quell uncomfortable emotions. But I still haven’t lost much more than five or 10 pounds from changing those behaviors.
That’s where gastric-bypass surgery comes in. It’s a drastic solution, but I have a drastic problem.I thought about it for four months before talking with my primary physician. I had discussions with my husband — who was against it for some time — my mom — who remains opposed — and a handful of close friends and relatives — all of whom are cautiously supportive.
I’ve had to discuss my decision with loved ones because they have a right to know, my employer because I will need a significant amount of time off and my health-care providers because their opinions determine whether my insurance company will cover the procedure.
I spent four months poring over research and patient accounts of the different types of surgery available. I devoted at least two months investigating my insurer’s policy on weight-loss surgery.
It’s a good thing I did that, too. Though there are a handful of different styles of weight-loss surgery performed in the United States, my health-maintenance organization only covers one — the Roux-en-Y gastric bypass, which I’ll discuss further in next week’s column.Gathering information on the procedure was daunting.
Actually, that’s a lie. Gathering information was easy; gathering information that can be understood by the average person was a different story.
When I first discussed gastric bypass with my doctor, he sent me home with a 60-page booklet published by my insurer that made my college biology textbook seem engaging. It took me a week of hard concentrating to plow through it, and I’m typically a fast reader.
I found my most useful information on the Internet.
Sure, not everything on the Web is credible, but there is a plethora of sites created by weight-loss surgery patients. One thing I’ve discovered is that WLS patients are part of a warm, welcoming community. For the most part, they have worked very hard to be successful and they want to help others do the same. There are also numerous Internet message boards that freely disseminate information and advice. Message boards are great because they are interactive; you can post questions and have them answered quickly. Finding out everything I could about surgical weight loss was important to me.
I’m almost embarrassed to admit it now, but I’ve been a vocal opponent of weight-loss surgery for a long time.Like many people, I thought surgery was a lazy way out. I knew it would be hard for me to explain to my loved ones why my tune suddenly changed. And it was important to me that I could justify it to myself.
Research helped me change my mind rather quickly. The first thing I discovered is that gastric bypass is far from a passive method of weight loss. Most bypass patients report spending more time planning their meals and exercising than ever before.
What I think makes surgical weight loss so much more effective than other methods is the rapid weight loss. Surgery patients are able to drop weight fast enough that exercise becomes easier on their bodies — which motivates and enables them to stick with it.That quick weight loss also serves as an emotionally motivating factor. It’s easier to feel successful when you can see your body changing before your own eyes.
I only finally decided that surgery was the option for me about a month ago. I spent about eight months weighing my options (no pun intended) and telling myself that I should try traditional methods one last time.
I’ve come to accept that traditional methods haven’t worked for me, and it’s time to try something else. It’s not going to be easy, but I’m willing to go through this in the hopes of one day becoming a mother — and a healthy one at that.
I’m officially under the gun to lose weight. I have obesity-related infertility, and if my husband and I hope to conceive the old fashioned way, I need to drop at least 100 pounds. And my doctor suggests I do it sooner rather than later. That’s no easy undertaking.After all, only 5 percent of Americans who diet are successful at maintaining weight loss. I’ve never been among that 5 percent — not even for a minute.
I’ve given up on the commercial weight-loss circuit. It’s not that I don’t believe Weight Watchers, Jenny Craig and similar programs are beneficial. I’ve spent seven years as a WW member, but I’ve never had any long-term success with those types of programs.
I’ve worked with three dieticians in the past two years. They succeeded in helping me improve my food choices and figure out meal planning. One has even helped me make a healthier transition to a pseudo-vegetarian lifestyle (I now abstain from red meat and poultry).But we never succeeded in the realm of weight loss.
I have worked with a couple of therapists on my issues with emotional/binge eating and had great success. It’s been at least six months since I’ve binged, and I no longer use food to quell uncomfortable emotions. But I still haven’t lost much more than five or 10 pounds from changing those behaviors.
That’s where gastric-bypass surgery comes in. It’s a drastic solution, but I have a drastic problem.I thought about it for four months before talking with my primary physician. I had discussions with my husband — who was against it for some time — my mom — who remains opposed — and a handful of close friends and relatives — all of whom are cautiously supportive.
I’ve had to discuss my decision with loved ones because they have a right to know, my employer because I will need a significant amount of time off and my health-care providers because their opinions determine whether my insurance company will cover the procedure.
I spent four months poring over research and patient accounts of the different types of surgery available. I devoted at least two months investigating my insurer’s policy on weight-loss surgery.
It’s a good thing I did that, too. Though there are a handful of different styles of weight-loss surgery performed in the United States, my health-maintenance organization only covers one — the Roux-en-Y gastric bypass, which I’ll discuss further in next week’s column.Gathering information on the procedure was daunting.
Actually, that’s a lie. Gathering information was easy; gathering information that can be understood by the average person was a different story.
When I first discussed gastric bypass with my doctor, he sent me home with a 60-page booklet published by my insurer that made my college biology textbook seem engaging. It took me a week of hard concentrating to plow through it, and I’m typically a fast reader.
I found my most useful information on the Internet.
Sure, not everything on the Web is credible, but there is a plethora of sites created by weight-loss surgery patients. One thing I’ve discovered is that WLS patients are part of a warm, welcoming community. For the most part, they have worked very hard to be successful and they want to help others do the same. There are also numerous Internet message boards that freely disseminate information and advice. Message boards are great because they are interactive; you can post questions and have them answered quickly. Finding out everything I could about surgical weight loss was important to me.
I’m almost embarrassed to admit it now, but I’ve been a vocal opponent of weight-loss surgery for a long time.Like many people, I thought surgery was a lazy way out. I knew it would be hard for me to explain to my loved ones why my tune suddenly changed. And it was important to me that I could justify it to myself.
Research helped me change my mind rather quickly. The first thing I discovered is that gastric bypass is far from a passive method of weight loss. Most bypass patients report spending more time planning their meals and exercising than ever before.
What I think makes surgical weight loss so much more effective than other methods is the rapid weight loss. Surgery patients are able to drop weight fast enough that exercise becomes easier on their bodies — which motivates and enables them to stick with it.That quick weight loss also serves as an emotionally motivating factor. It’s easier to feel successful when you can see your body changing before your own eyes.
I only finally decided that surgery was the option for me about a month ago. I spent about eight months weighing my options (no pun intended) and telling myself that I should try traditional methods one last time.
I’ve come to accept that traditional methods haven’t worked for me, and it’s time to try something else. It’s not going to be easy, but I’m willing to go through this in the hopes of one day becoming a mother — and a healthy one at that.
Saturday, December 11, 2004
Drastic measures for drastic times

Originally published Dec. 11, 2004, in the Tracy Press.
Few souls would embark on a weight-loss plan in the middle of the holiday season.
Fewer still would do so publicly, as I’m about to do. My journey is different from many in that I’m opting for a drastic solution to my weight problem — gastric-bypass surgery. Contrary to the belief of some, including myself at first, deciding to go under the knife is not an easy choice to make. In fact, it’s the hardest decision I’ve ever made. But I’ve come to realize it’s the only choice I have.
For me, this isn’t about fitting into a certain size or looking good in a bikini. Two decades of obesity has ensured that I will never look good in a bathing suit. This is about my health. I have been overweight for as long as I can remember. My size was encouraged. I remember being praised by the school lunchroom attendant for always eating all of my food. The idea of “bigger is better” was ingrained in my family. I was praised when I gained weight or outgrew a size. I was a happy kid with a bulging belly and chunky thighs.
By the third grade, I weighed 111 pounds. It didn’t occur to me that anything was wrong with that until a teacher asked if I wanted her to remove my weight from the classroom biographical chart. I had no idea until I saw that chart that most of my classmates weighed 60 to 70 pounds. Of course, that’s about the time that playing tag and hide-and-seek stopped appealing to me. I preferred instead to read books during recess or trade Garbage Pail Kids cards with my friends. I was teased a lot, but those memories are vague. As an only child, I didn’t have any siblings to motivate me to be active, either. It was just me and my mom — who was overweight herself — keeping each other company. By the fifth grade, I was about 5 feet tall and weighed 199 pounds. That weight on a 21-year-old woman equates to a body mass index of 38 — or severely obese.
If my life has been a war with obesity, the fifth grade is when I first engaged in battle.
By this time, I understood that I looked different than other kids. I couldn’t buy the same clothes in the same stores as the cool kids, and keeping my ever-expanding body in clothes was an expensive endeavor at best. I made up my mind that I would not gain any more weight. I almost succeeded. I did fairly well maintaining my weight from fifth grade through high school, graduating at about 205 pounds.
I wish I could say the same about my college years. By the time I graduated from college, I had packed on another 100 pounds doing nothing in particular — though I’m sure my stints working in fast food and my own casual dining didn’t help. Five years later, I’ve added even more to my 5-foot, 4- inch frame. My body mass index, or BMI, is now 56, well above being morbidly obese.
According to the BMI chart on ObesityHelp, I’m “super obese.” Maybe I should buy a cape and some queen-size tights.
Any way you look at it, I’ve been severely obese for 20 years. The problem is that the consequences have finally begun to catch up with me. I have high blood pressure, bad knees, a bad hip and problems with fluid retention — and I’m only 27.
I’ve tried just about every diet and exercise program on the market, with minimal success.Even after trying — and failing — each program, I still didn’t feel like I had tried everything. I figured my failures were symptoms of a greater character flaw. I would tell myself that once I was truly fed up with the weight, I would find a method, stick to it and be able to be fit and healthy, once and for all.
That day of being fed up finally came earlier this year, though not in the way I expected. I imagined it would come after I had children and was frustrated with lugging around babies and “baby weight.” But instead it came in an OB/GYN’s office when I was diagnosed with obesity-r-elated infertility.That’s when my weight stopped being about me, and I realized how my battle with obesity affected those around me, particularly my husband and our future family.
Obesity-related infertility isn’t uncommon. Stored fat also holds stored estrogen, and when you have lots of stored fat, all that estrogen confuses your reproductive system.
Doctors can prescribe drugs to trick the body into ignoring the excess estrogen or force the body to ovulate. Or they can perform artificial insemination and fertilization procedures.
But to me, it just doesn’t make sense to combat this obesity-related hormone imbalance with more hormones. All of those prescriptions and procedures seem more like a Band-Aid than anything else.
After all, if getting my fertility back — if I ever had it to begin with — is as simple as losing weight, why not just solve the basic problem of obesity?
Few souls would embark on a weight-loss plan in the middle of the holiday season.
Fewer still would do so publicly, as I’m about to do. My journey is different from many in that I’m opting for a drastic solution to my weight problem — gastric-bypass surgery. Contrary to the belief of some, including myself at first, deciding to go under the knife is not an easy choice to make. In fact, it’s the hardest decision I’ve ever made. But I’ve come to realize it’s the only choice I have.
For me, this isn’t about fitting into a certain size or looking good in a bikini. Two decades of obesity has ensured that I will never look good in a bathing suit. This is about my health. I have been overweight for as long as I can remember. My size was encouraged. I remember being praised by the school lunchroom attendant for always eating all of my food. The idea of “bigger is better” was ingrained in my family. I was praised when I gained weight or outgrew a size. I was a happy kid with a bulging belly and chunky thighs.
By the third grade, I weighed 111 pounds. It didn’t occur to me that anything was wrong with that until a teacher asked if I wanted her to remove my weight from the classroom biographical chart. I had no idea until I saw that chart that most of my classmates weighed 60 to 70 pounds. Of course, that’s about the time that playing tag and hide-and-seek stopped appealing to me. I preferred instead to read books during recess or trade Garbage Pail Kids cards with my friends. I was teased a lot, but those memories are vague. As an only child, I didn’t have any siblings to motivate me to be active, either. It was just me and my mom — who was overweight herself — keeping each other company. By the fifth grade, I was about 5 feet tall and weighed 199 pounds. That weight on a 21-year-old woman equates to a body mass index of 38 — or severely obese.
If my life has been a war with obesity, the fifth grade is when I first engaged in battle.
By this time, I understood that I looked different than other kids. I couldn’t buy the same clothes in the same stores as the cool kids, and keeping my ever-expanding body in clothes was an expensive endeavor at best. I made up my mind that I would not gain any more weight. I almost succeeded. I did fairly well maintaining my weight from fifth grade through high school, graduating at about 205 pounds.
I wish I could say the same about my college years. By the time I graduated from college, I had packed on another 100 pounds doing nothing in particular — though I’m sure my stints working in fast food and my own casual dining didn’t help. Five years later, I’ve added even more to my 5-foot, 4- inch frame. My body mass index, or BMI, is now 56, well above being morbidly obese.
According to the BMI chart on ObesityHelp, I’m “super obese.” Maybe I should buy a cape and some queen-size tights.
Any way you look at it, I’ve been severely obese for 20 years. The problem is that the consequences have finally begun to catch up with me. I have high blood pressure, bad knees, a bad hip and problems with fluid retention — and I’m only 27.
I’ve tried just about every diet and exercise program on the market, with minimal success.Even after trying — and failing — each program, I still didn’t feel like I had tried everything. I figured my failures were symptoms of a greater character flaw. I would tell myself that once I was truly fed up with the weight, I would find a method, stick to it and be able to be fit and healthy, once and for all.
That day of being fed up finally came earlier this year, though not in the way I expected. I imagined it would come after I had children and was frustrated with lugging around babies and “baby weight.” But instead it came in an OB/GYN’s office when I was diagnosed with obesity-r-elated infertility.That’s when my weight stopped being about me, and I realized how my battle with obesity affected those around me, particularly my husband and our future family.
Obesity-related infertility isn’t uncommon. Stored fat also holds stored estrogen, and when you have lots of stored fat, all that estrogen confuses your reproductive system.
Doctors can prescribe drugs to trick the body into ignoring the excess estrogen or force the body to ovulate. Or they can perform artificial insemination and fertilization procedures.
But to me, it just doesn’t make sense to combat this obesity-related hormone imbalance with more hormones. All of those prescriptions and procedures seem more like a Band-Aid than anything else.
After all, if getting my fertility back — if I ever had it to begin with — is as simple as losing weight, why not just solve the basic problem of obesity?
Subscribe to:
Posts (Atom)